 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
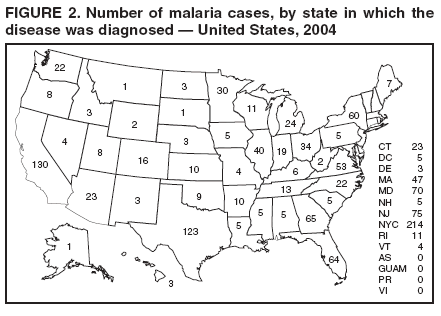
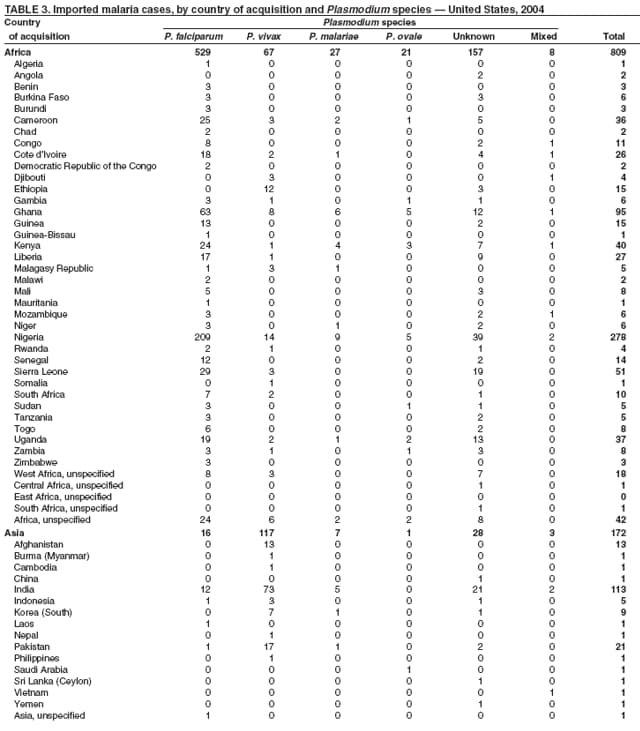
Malaria Surveillance --- United States, 2004Jacek Skarbinski, MD,1,2 M. James Eliades,
MD,1,2 Louise M. Causer,
MBBS,2 Ann M. Barber,2 Sonja Mali,
MPH,2 Phuc Nguyen-Dinh, MD,2 Jacquelin M. Roberts,
MS,2 Monica E. Parise, MD,2 Laurence Slutsker,
MD,2 Robert D. Newman, MD2
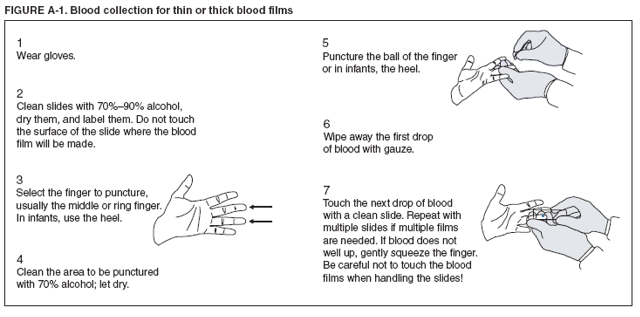
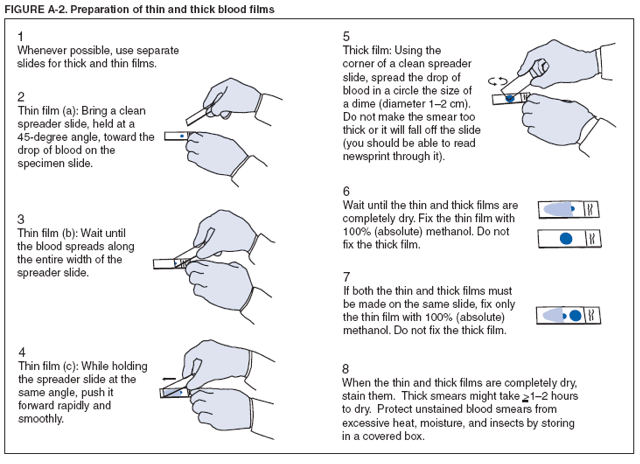
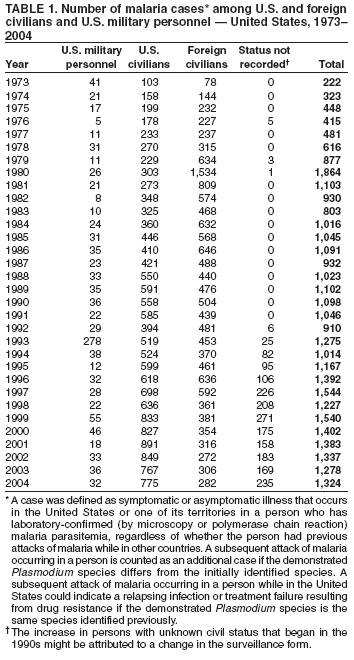
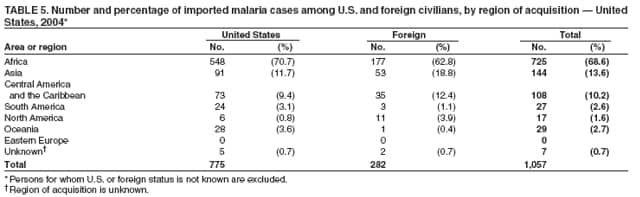
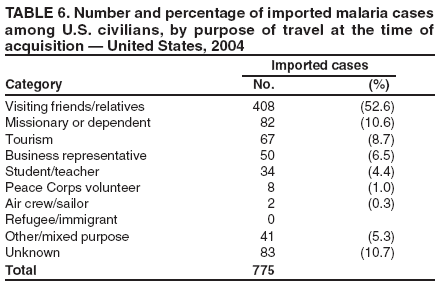
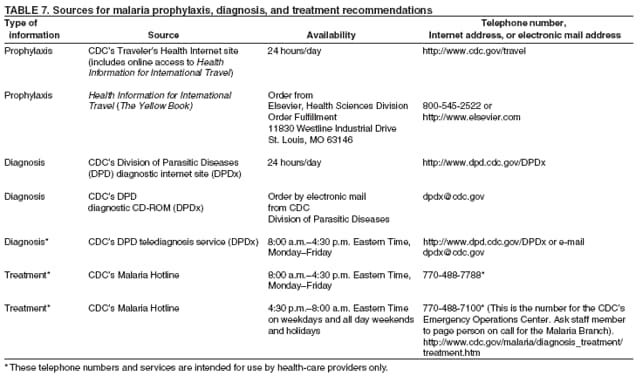
Corresponding author: Jacek Skarbinski, MD, National Center for Infectious Diseases, 1600 Clifton Road, NE, MS F-22, Atlanta, GA 30333. Telephone: 770-488-7785; Fax: 770-488-4206; E-mail: jskarbinski@cdc.gov. AbstractProblem/Condition: Malaria in humans is caused by any of four species of intraerythrocytic protozoa of the genus Plasmodium (i.e., P. falciparum, P. vivax, P. ovale, or P. malariae). These parasites are transmitted by the bite of an infective female Anopheles sp. mosquito. The majority of malaria infections in the United States occur among persons who have traveled to areas with ongoing malaria transmission. In the United States, cases can occur through exposure to infected blood products, congenital transmission, or local mosquitoborne transmission. Malaria surveillance is conducted to identify episodes of local transmission and to guide prevention recommendations for travelers. Period Covered: This report summarizes cases in persons with onset of illness in 2004 and summarizes trends during previous years. Description of System: Malaria cases confirmed by blood film are mandated to be reported to local and state health departments by health-care providers or laboratory staff. Case investigations are conducted by local and state health departments, and reports are transmitted to CDC through the National Malaria Surveillance System (NMSS). Data from NMSS serve as the basis for this report. Results: CDC received reports of 1,324 cases of malaria, including four fatal cases, with an onset of symptoms in 2004 among persons in the United States or one of its territories. This number represents an increase of 3.6% from the 1,278 cases reported for 2003. P. falciparum, P. vivax, P. malariae, and P. ovale were identified in 49.6%, 23.8%, 3.6%, and 2.0% of cases, respectively. Seventeen patients (1.3% of total) were infected by two or more species. The infecting species was unreported or undetermined in 262 (19.8%) cases. Compared with 2003, the number of reported malaria cases acquired in the Americas (n = 173) increased 17.7%, whereas the number of cases acquired in Asia (n = 172) and Africa (n = 809) decreased 2.8% and 3.7%, respectively. Of 775 U.S. civilians who acquired malaria abroad, only 160 (20.6%) reported that they had followed a chemoprophylactic drug regimen recommended by CDC for the area to which they had traveled. Four patients became infected in the United States; three cases were attributed to congenital transmission and one to laboratory-related mosquitoborne transmission. Four deaths were attributed to malaria, including two caused by P. falciparum, one by P. vivax, and one by a mixed infection with P. falciparum and P. malariae. Interpretation: The 3.6% increase in malaria cases in 2004, compared with 2003, resulted primarily from an increase in the number of cases acquired in the Americas but was offset by a decrease in the number of cases acquired in Africa and Asia. This limited increase might reflect local changes in disease transmission, increased travel to regions in which malaria is endemic, or fluctuations in reporting to state and local health departments. These changes likely reflect expected variation in annual reporting and should not be interpreted as indicating a longer-term trend. In the majority of reported cases, U.S. civilians who acquired infection abroad had not adhered to a chemoprophylaxis regimen that was appropriate for the country in which they acquired malaria. Public Health Actions: Additional investigations were conducted for the four fatal cases and four infections acquired in the United States. Persons traveling to a malarious area should take one of the recommended chemoprophylaxis regimens appropriate for the region of travel and use personal protection measures to prevent mosquito bites. Any person who has been to a malarious area and who subsequently has a fever or influenza-like symptoms should seek medical care immediately and report their travel history to the clinician; investigation should include a blood-film test for malaria. Malaria infections can be fatal if not diagnosed and treated promptly. Recommendations concerning malaria prevention can be obtained from CDC at http://www.cdc.gov/travel or by calling the Malaria Hotline at telephone 770-488-7788. Recommendations concerning malaria treatment can be obtained at http://www.cdc.gov/malaria/diagnosis_treatment/treatment.htm or by calling the Malaria Hotline. IntroductionMalaria in humans is caused by infection with one or more of four species of Plasmodium (i.e., P. falciparum, P. vivax, P. ovale, and P. malariae) that can infect humans. Other Plasmodium species infect animals. The infection is transmitted by the bite of an infective female Anopheles sp. mosquito. Malaria remains a devastating global problem, with an estimated 350--500 million cases occurring annually (1). Forty-nine percent of the world's population lives in areas where malaria is transmitted (e.g., parts of Africa, Asia, the Middle East, Eastern Europe, Central and South America, Hispaniola, and Oceania), and approximately 1 million persons die from malaria each year, 80% of them in sub-Saharan Africa (1). Before the 1950s, malaria was endemic throughout the southeastern United States; an estimated 600,000 cases occurred in 1914 (2). During the late 1940s, a combination of improved housing and socioeconomic conditions, water management, vector-control efforts, and case management was successful at interrupting malaria transmission in the United States. Since then, malaria case surveillance has been maintained to detect locally acquired cases that could indicate the reintroduction of transmission and to monitor patterns of resistance to antimalarial drugs. Anopheline mosquitoes remain seasonally present in all states except Hawaii. The majority of reported cases of malaria diagnosed each year in the United States are imported from regions where malaria transmission is known to occur, although congenital infections and infections resulting from exposure to blood or blood products are also reported in the United States. In addition, a limited number of cases are reported that might have been acquired through local mosquitoborne transmission (3). State and local health departments and CDC investigate malaria cases acquired in the United States, and CDC analyzes data from imported cases to detect trends in acquisition. This information is used to guide malaria prevention recommendations for international travelers. For example, an increase in P. falciparum malaria among U.S. travelers to Africa, an area with increasing chloroquine resistance, prompted CDC to change the recommended chemoprophylaxis regimen from chloroquine to mefloquine in 1990 (4). The signs and symptoms of malaria illness are varied, but the majority of patients have fever. Other common symptoms include headache, back pain, chills, increased sweating, myalgia, nausea, vomiting, diarrhea, and cough. The diagnosis of malaria should be considered for persons with these symptoms who have traveled to an area with known malaria transmission. Malaria also should be considered in the differential diagnosis of persons who have fever of unknown origin, regardless of their travel history. Untreated P. falciparum infections can rapidly progress to coma, renal failure, pulmonary edema, and death. This report summarizes malaria cases reported to CDC regarding persons with onset of symptoms in 2004. MethodsData SourcesMalaria case data are reported to the National Malaria Surveillance System (NMSS) and the National Notifiable Diseases Surveillance System (NNDSS) (5). Although both systems rely on passive reporting, the numbers of reported cases might differ because of differences in collection and transmission of data. A substantial difference in the data collected in these two systems is that NMSS receives more detailed clinical and epidemiologic data regarding each case (e.g., information concerning the area to which the infected person has traveled). This report presents only data regarding cases reported to NMSS. Cases of blood-film--confirmed malaria among civilians and military personnel are identified by health-care providers or laboratories. Each confirmed malaria case is reported to local or state health departments and to CDC on a uniform case-report form that contains clinical, laboratory, and epidemiologic information. CDC staff review all report forms when received and request additional information from the provider or the state, if necessary (e.g., when no recent travel to a malarious country is reported). Reports of other cases are telephoned to CDC directly by health-care providers, usually when they are seeking assistance with diagnosis or treatment. Information regarding cases reported directly to CDC is shared with the relevant state health department. All cases that have been acquired in the United States are investigated, including all induced and congenital cases and possible introduced or cryptic cases. Information derived from uniform case report forms is entered into a database and analyzed annually. DefinitionsThe following definitions are used in this report:
|