|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
Using Tandem Mass Spectrometry for Metabolic Disease Screening Among NewbornsA Report of a Work Group The following CDC staff members prepared this report: W. Harry Hannon, Ph.D. in collaboration with William J. Becker, D.O. Donald H. Chace, Ph.D., M.S.F.S. George C. Cunningham, M.D. George F. Grady, M.D. Gary L. Hoffman Marie Y. Mann, M.D., M.P.H. Joseph Muenzer, M.D., Ph.D. John J. Mulvihill, M.D. Susan R. Panny, M.D. "Public health agencies (federal and state), in partnership
with health professionals and consumers, should continue to develop
and evaluate innovative testing technologies [and] design and apply
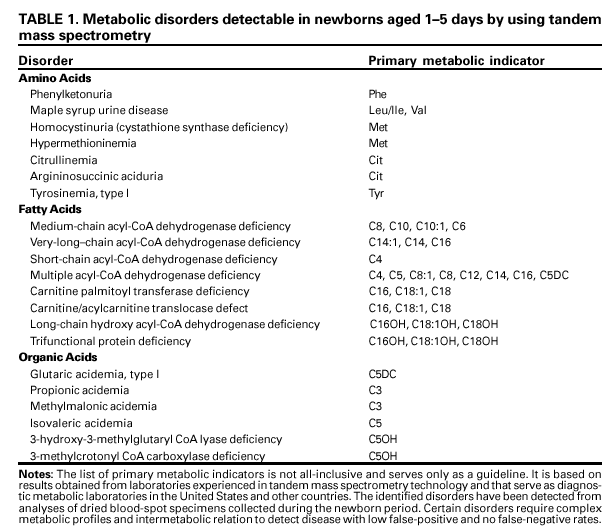
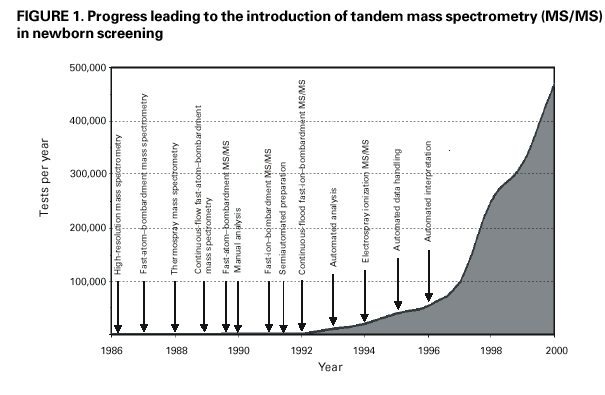
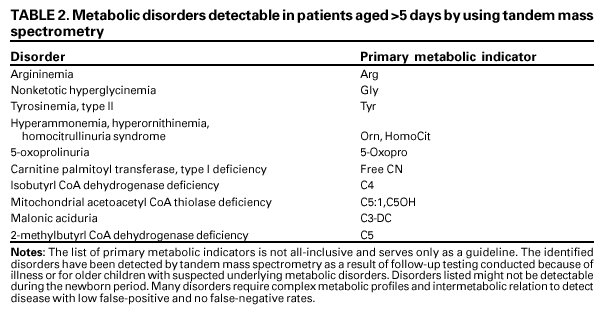
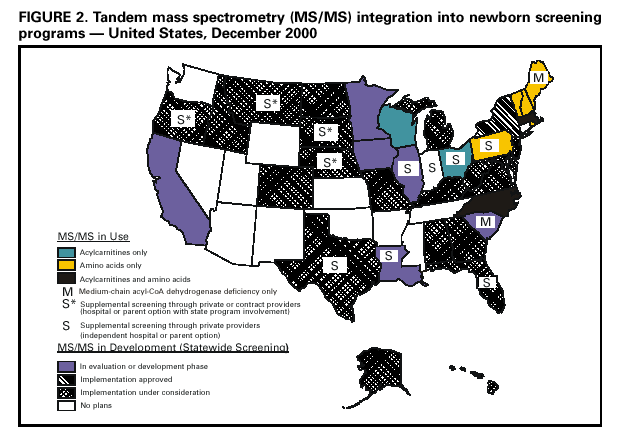
minimum standards for newborn screening activities . . . ." Summary Increasingly, tandem mass spectrometry (MS/MS) is being used for newborn screening because this laboratory testing technology substantially increases the number of metabolic disorders that can be detected from dried blood-spot specimens. In June 2000, the National Newborn Screening and Genetics Resource Center, in collaboration with CDC and the Health Resources and Services Administration, convened a workshop in San Antonio, Texas. Workshop participants examined programmatic concerns for health providers choosing to integrate MS/MS technology into their newborn screening activities. Representatives from approximately 50 public and private health agencies and universities participated in the workshop. The workshop participants and work group focused on laboratory methodology, decision criteria, quality assurance, diagnostic protocols, patient case management, and program evaluation for using MS/MS to analyze dried blood spots routinely collected from newborns. This work group report contains proposals for planning, operating, and evaluating MS/MS technology in newborn screening and maternal and child health programs. As a supplement to these proposals, this report contains synopses of selected presentations made at the 2000 workshop regarding integration of MS/MS technology into newborn screening programs. The proposals contained in this report should assist policymakers, program managers, and laboratorians in making informed decisions regarding the process of including MS/MS technology in their newborn screening and maternal and child health programs. INTRODUCTIONEach year, approximately 4 million babies in the United States have dried blood spots analyzed through newborn* screening programs. This screening is intended to detect inborn disorders that can result in early mortality or lifelong disability. Detectable disorders include metabolic disorders (e.g., phenylketonuria [PKU]), hematologic disorders (e.g., sickle cell disease), and endocrinopathies (e.g., congenital hypothyroidism). These three groups of disorders account for approximately 3,000 new cases of potentially fatal or debilitating disease each year for which outcomes are improved with early identification and treatment through newborn screening systems. The introduction of tandem mass spectrometry (MS/MS) in the 1990s for population-based newborn screening has enabled health-care providers to detect an increased number of metabolic disorders in a single process by using dried blood-spot specimens routinely collected from newborns (13). However, using MS/MS in newborn screening programs is new, and scientific data are limited regarding incorporating this technology into newborn screening and maternal and child health programs. MS/MS technology enables improvements in and consolidation of metabolic screening methods to detect amino acid disorders (e.g., PKU, maple syrup urine disease, and homocystinuria) among newborns, and does so with a low false-positive rate (46). MS/MS technology expands the metabolic disorder screening panel (i.e., the number of disorders that can be detected) by incorporating an acylcarnitine profile, which enables detection of fatty acid oxidation disorders (e.g., medium-chain acyl-CoA dehydrogenase [MCAD] deficiency) (7-10) and other organic acid disorders. MS/MS can reliably analyze approximately 20 metabolites in one short-duration run (i.e., ~2 minutes) and provide a comprehensive assessment from a single blood-spot specimen (Table 1). Screening for multiple disorders in a single analytical run by using MS/MS requires that program administrators and laboratorians choose which types of conditions are to be screened. For example, laboratory A uses MS/MS to detect amino acids only; laboratory B uses MS/MS to detect acylcarnitines only; and laboratory C screens for both. In addition, other technical concerns must be addressed before MS/MS technology can be integrated effectively into a newborn screening program, including deciding which analytes to use in characterizing each disorder (e.g., octanoylcarnitine analysis can indicate both MCAD deficiency and multiple acyl-CoA dehydrogenase deficiency). Studies are limited regarding use of MS/MS technology in newborn screening programs, but existing studies indicate that screening a full panel of acylcarnitines and amino acids yields rates of 1:4,0001:5,000 for MS/MS-detectable disorders (16-13). For certain metabolic disorders, early detection can result in substantial improvements in health outcomes. For example, MCAD, which has an incidence rate of 1:10,0001:20,000 newborns, results in substantial morbidity and reported mortality rates of 20%25% among infants and children during the first 3 years of life (14). Effective treatment is available, and detection and intervention before onset of illness can prevent mortality and improve the quality of life for MCAD patients. Although effective treatments do not exist yet for certain other metabolic disorders identifiable by MS/MS testing (1), patient and family advantages can still be achieved through early diagnosis (15). Also, MS/MS can detect metabolic disorders after an illness occurs, even if that illness occurs after the newborn period (Table 2). June 2000 Workshop and Work Group Goals In June 2000, the National Newborn Screening and Genetics Resource Center, in collaboration with CDC and the Health Resources and Services Administration (HRSA), convened a workshop in San Antonio, Texas, to examine programmatic concerns for effectively integrating MS/MS technology into newborn screening programs. Representatives from approximately 50 public and private health agencies and universities participated in the workshop.** The participants focused on laboratory methodology, decision criteria, quality assurance, diagnostic protocols, patient case management, and program evaluation. This report contains their proposals for planning, operating, and evaluating MS/MS technology in newborn screening and maternal and child health programs. Their proposals are included in this report to assist policymakers, program managers, and laboratorians in planning state-mandated screening programs or optional metabolic testing through partnering of state and private screening laboratories. The workshop participants did not address newborn disorders that are screened by other technologies and that should be considered for a comprehensive newborn screening panel (e.g., sickle cell disease, congenital adrenal hyperplasia, galactosemia, biotinidase deficiency, and cystic fibrosis). Therefore, these proposals address MS/MS technology only. Further, as a supplement to their proposals, this report contains synopses of selected presentations made at the 2000 workshop regarding integration of MS/MS technology into newborn screening programs (Appendix). Specifically, workshop participants focused on the following concerns for policymakers, program managers, and laboratorians interested in MS/MS testing for newborn screening programs:
|