Are Women with Recent Live Births Aware of the Benefits of Folic Acid?
Indu B. Ahluwalia, M.P.H., Ph.D.
Division of Reproductive Health
National Center for Chronic Disease Prevention and Health Promotion
Katherine Lyon Daniel, Ph.D.
National Center on Birth Defects and Developmental Disabilities
Summary
Each year, approximately 4,000 pregnancies result in spina bifida
or anencephaly, serious and often fatal conditions for the newborn. The
B vitamin folic acid can reduce the incidence of these conditions by
50%--70%. To examine folic acid awareness among women who had recently delivered
a live-born infant, CDC analyzed Pregnancy Risk Assessment Monitoring
System (PRAMS) data for 1995--1998. The question used to measure awareness
was, "Have you ever heard or read that taking the vitamin folic acid can
help prevent some birth defects?" During the study period, overall folic
acid awareness increased 15%, from 64% in 1996 to 73% in 1998, although
changes varied by state. Despite this increase, differences in folic acid awareness
were observed among different groups of women. Women who obtained a
high school education or less; who were black, Hispanic, or from other
racial/ethnic groups; who entered prenatal care after the first trimester; and
whose pregnancies were unintended were less aware of folic acid.
This study indicates that gaps persist among women in low
socioeconomic groups. Overall, PRAMS data indicated an increase in folic acid
awareness among women with recent deliveries. However, this awareness might be
too late for the pregnancy that has occurred, indicating a continued need
to educate all reproductive-aged women regarding the need to take folic
acid before they become pregnant.
BACKGROUND
Approximately 4,000 pregnancies are affected by neural tube birth defects
each year in the United States (1). These conditions are serious defects in the formation
of the brain and spine that are either fatal or have long-term health consequences.
The formation of the neural tube occurs early in pregnancy --- in many cases, before
a woman realizes she is pregnant and long before her first prenatal
visit. Approximately 50% of neural tube defects are cases of anencephaly, in which
the infant's brain is completely or partially missing, and these infants die before
or shortly after birth. The other half of cases are spina bifida, which is a malformation
of
the spinal column that causes the spinal cord to form outside the
protective backbone. Most children with spina bifida need numerous surgeries and
experience problems throughout their lives, including paralysis, bowel or bladder
incontinence, and learning disabilities. The social and economic costs of these conditions are
high (2,3).
Research has demonstrated that periconceptional intake of 0.4 mg of the
B vitamin folic acid reduces the risk for neural tube defects 50%--70%
(4--8). Periconceptional multivitamin use can also reduce the risk for other defects
(e.g., orofacial clefts, conotruncal heart defects, and urinary tract defects)
(9--11). In response to the findings that folic acid can prevent neural tube defects,
several national initiatives were implemented. In 1992, the U.S. Public Health Service
(PHS) recommended that all women capable of becoming pregnant consume 0.4 mg
of folic acid per day to reduce the risk for neural tube defects
(12). In 1996, the U.S. Food and Drug Administration (FDA) mandated that all enriched cereal
grain products be fortified with folic acid beginning in January 1998
(13). In April 1998, the Food and Nutrition Board of the National Academy of Sciences recommended that
all women of reproductive age consume 400 micrograms of synthetic folic acid
daily from supplements or fortified foods, in addition to folate found naturally in
foods (14). Healthy People 2010 includes national objectives to increase folic
acid consumption, increase red blood cell folate levels, and measure decreases in
birth defects (15). Recent research has demonstrated that fortification and other
health promotion efforts have caused a mean increase in blood folate levels among
women of childbearing age (16--19). Given the association between folic acid
consumption and reduction in neural tube defects and other birth defects, higher folate
levels could reduce adverse birth outcomes in the United States
(19,20). Many organizations and groups (e.g., CDC, March of Dimes) encourage clinicians
and health-care providers to counsel reproductive-aged women regarding the need
for periconceptional supplementation use to prevent neural tube defects
(20--23). Despite these efforts, this information is apparently not getting to women
of childbearing age quickly enough. An open-ended survey conducted by the
Gallup Organization in 1998 for the national March of Dimes indicated that
only approximately 13% of all women of childbearing age can spontaneously recall
that folic acid can prevent birth defects, and even fewer (7%) know that folic acid must
be consumed before pregnancy to provide this benefit
(1,24,25). Based on surveys conducted in 1996 and 1997, the Behavioral Risk Factor Surveillance System
(BRFSS) reported that approximately 35% of reproductive-aged women queried
could correctly identify the purpose of folic acid from among four choices
(26). The BRFSS is a state-based, random-digit--dialed telephone survey of the
noninstitutionalized U.S. population aged
>18 years.
This study sought to build on past research and promotion efforts by
identifying changes and gaps in folic acid awareness among women who had recently
delivered a live-born infant in the states that participate in the Pregnancy Risk
Assessment Monitoring System (PRAMS). The specific research questions guiding this
analysis were as follows:
Has there been a change in women's awareness regarding folic acid use?
How do the estimates of folic acid awareness among this population
compare with estimates from national surveys (e.g., the March of Dimes survey
and
BRFSS)?
Are there specific gaps that remain to be addressed in folic acid
awareness among women who have recently given birth to a live-born infant and who
are potentially at risk for future pregnancies, whether intended or unintended?
METHODS
Data
This study examined women's awareness regarding folic acid using data
from PRAMS, which collects information on maternal behaviors and experiences
during pregnancy from projects in 24 states* and New York City. Each month,
PRAMS selects a stratified, systematic sample of 100--250 women who have recently
given birth in a particular area from the birth certificates of the infants, and a
survey questionnaire is mailed to the selected mothers approximately 2--6 months
after delivery. Several attempts are made to contact the mother by mail. If that fails,
the mother is contacted by telephone, and an attempt is made to interview her.
The survey questionnaire is linked back to a select set of items from the birth
certificate. The overall data are statistically weighted to adjust for the survey
design, noncoverage, and nonresponse. Details of the methods and populations surveyed
by PRAMS are provided elsewhere (27).
The current study used multiple years of data (1995--1998) from 13
states (n=58,625 births), with response rates ranging from 68% to >80%. Data
from Alabama, Alaska, Arkansas, Colorado, Florida, Georgia, Maine, New York
(excluding New York City), North Carolina, Oklahoma, South Carolina, Washington, and
West Virginia were used. Because all of these states did not initiate data collection at
the same time, earlier years of data did not exist for some states; for Georgia, no
1998 data were available. These states were chosen for analysis because they had
the most years of data on folic acid awareness and adequate response rates to
answer the research questions.
To define the measures used in this analysis, questions from the PRAMS
survey and specific variables from birth certificates were used. The primary measure ---
folic acid awareness --- was defined as women's responses to the following
question: "Have you ever heard or read that taking the vitamin folic acid can help
prevent some birth defects?" Response options were "yes" or "no." Reported race
was classified as black, white, or other, and ethnicity was classified as either Hispanic
or non-Hispanic. Education status was classified as less than high school, high
school completion, or more than high school. Maternal age was divided into four
categories (<19, 20--29, 30--39, and
>40 years). Marital status was categorized as married or
not married. Women who had >1 child were categorized as multipara, whereas those
for whom the index birth was the first were categorized as primipara. Women
who stated that they had insurance before they became pregnant were categorized
as having insurance, and those who answered no were classified as not having
any insurance before pregnancy. Women were asked what type of insurance paid
for
their prenatal care, with categories listed as Medicaid, private, and other.
Enrollment in Medicaid or the Special Supplemental Nutrition Program for Women, Infants,
and Children (WIC) was categorized as a dichotomous variable. Choices for place
of prenatal care were hospital, health department, private doctor, Indian Health
Service or other federally funded program, and other. In addition to demographic,
health-care provider, and insurance variables, this study also examined women's
pregnancy intention status, timing of prenatal-care initiation, and whether the
prenatal-care provider discussed nutrition and the baby's growth and development.
Women's pregnancy intentions were divided into four categories --- pregnancy was
intended sooner, pregnancy was intended to occur at the time it did, pregnancy was
intended for a later time, or pregnancy was not intended. Initiation of prenatal care
was defined as entry into prenatal care during the first trimester or later/none.
Women who had not obtained any prenatal care were put into the latter category.
Whether women received professional advice on what to eat during pregnancy and
whether their provider discussed fetal growth and development were defined as yes or no.
Software for Survey Data Analysis (SUDAAN) (Version 7.0; Research
Triangle Institute, Research Triangle Park, North Carolina) was used for data analysis
to ensure that the standard error estimates reflected the PRAMS survey design.
Multiple logistic regression was used to examine overall gaps in folic acid awareness.
RESULTS
During 1995--1998, folic acid awareness increased overall and in most of
the states in this analysis. The major shift appears to have occurred during
1996--1997 (Figure). Change in folic acid awareness is particularly noteworthy for the 10
states with data before 1997 (e.g., the percentage change in South Carolina was 27%
during 1995--1998). However, not all states had large increases (e.g., the change
in Washington was only 5% during 1996--1998), nor were all changes positive (Table 1). In 1998, the most recent year for which data were available, folic acid
awareness ranged from 66.4% (95% confidence intervals [CI]=63.5%--69.3%) in Arkansas
to 83.4% (95% CI=81.0%--85.7%) in Maine.
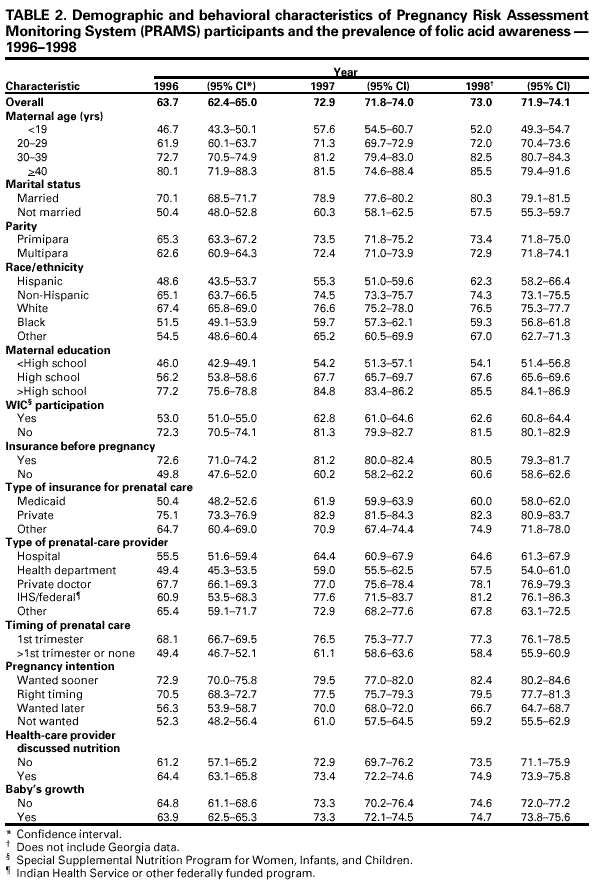
This study also examined folic acid awareness for 3 years (1996--1998),
using certain demographic and prenatal-care characteristics, for all 13 states
combined (Table 2). Prevalence estimates indicated an increase in folic acid awareness
during 1996--1997 among all groups, although this increase appeared to level off
during 1997--1998. Despite the overall increases, prevalence estimates remained
lower among women who were younger; were not married; were black and Hispanic; had
a high school education or less; were participating in WIC or received money
from Medicaid for prenatal care; had no insurance before becoming pregnant; did
not intend to become pregnant; began their prenatal care after the first trimester;
and received prenatal care from the health department (Table 2).
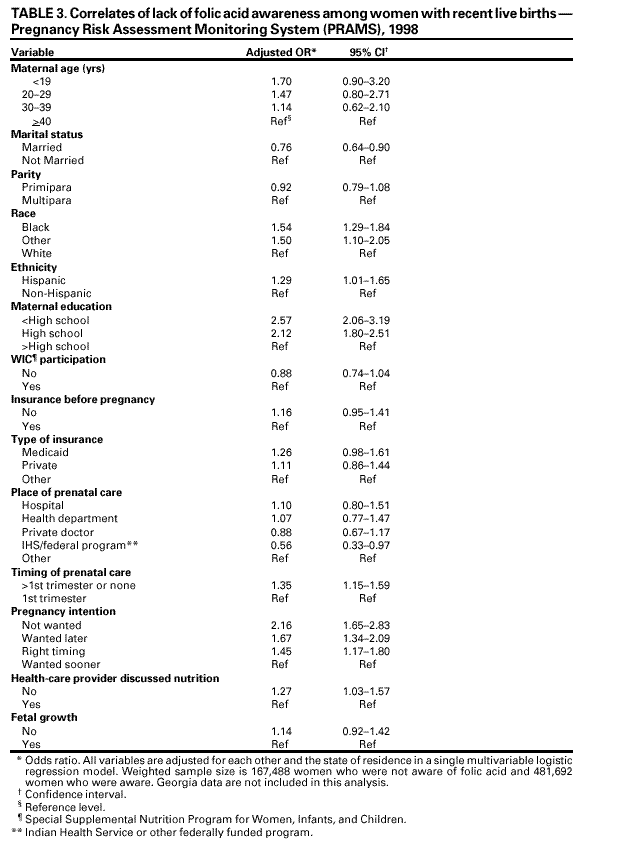
The 1998 data were used to examine the correlates of folic acid awareness
among women with recent live births. Multivariable analyses of these data indicated
that women with a high school education or less and women who did not want to
be pregnant at all were more than twice as likely to be unaware of the benefits of
folic acid (Table 3). Compared with women who wanted their pregnancies to occur
sooner,
those who wanted their pregnancies then or later were also less likely to know
about folic acid. Women who were black, Hispanic, or from other racial/ethnic groups,
as well as those who entered prenatal care later than the first trimester or had no
care and those whose providers did not discuss nutrition during prenatal visits
were significantly less likely to be aware of the benefits of taking folic acid to
prevent certain birth defects (Table 3). Women who were married and who reported that
their place of prenatal care was the Indian Health Service or another federally
funded program were more likely to know about folic acid.
DISCUSSION
PRAMS data indicate that women's awareness regarding folic acid use
has increased since 1995--1996, with the level of increase varying by state. These
findings suggest that health promotion efforts are working, albeit slowly in some
populations, and that more women became aware of the benefits of folic acid during
1996--1998. Several national campaigns were implemented during the early to
mid-1990s, including a March of Dimes campaign called Think Ahead in 1995. The Think
Ahead campaign was designed to promote folic acid awareness through multiple
channels (e.g., professional and public education, media campaigns, advertisements), and
its efforts were supplemented by state initiatives designed to promote awareness
and consumption of foods containing or fortified with folic acid
(28). In 1997, the Florida Department of Citrus began to promote folic acid intake through consumption
of orange juice, using paid television and radio advertisements, and this campaign
was cited most often by 1998 focus group participants
(29). PRAMS data also indicate that states with folic acid awareness data before 1996 reported a greater increase
in awareness compared with those that did not. This finding suggests that
national efforts coupled with state and local efforts to promote folic acid awareness could
be contributing to this increase. In 1997, the National Council on Folic Acid (NCFA)
was established to expand education efforts to both women and health professionals
by working in partnership with local and state coalitions. NCFA consists of
professional associations, maternal and child health advocacy groups, and
community-based health organizations that have implemented education and folic acid
awareness campaigns among their own memberships, as well as with
reproductive-aged women (30). NCFA developed targeted messages for women intending pregnancy
as well as for those capable of becoming pregnant who might not intend to
become pregnant, given that 50% of pregnancies in the United States are unplanned
(30,31). More information on NCFA is available on the Internet at
<http://www.cdc.gov/ncbddd/folicacid/council/htm>.
PRAMS findings on folic acid awareness among women of childbearing age
are similar to national estimates published by the March of Dimes from its 1998
survey of women aged 18--45 years. The March of Dimes reported that folic acid
awareness increased from 52% in 1995 to 66% in 1997 to 68% in 1998 and to 75% in 2000 ---
an overall increase of 44% (1,24,25). At the same time, consumption of
vitamins containing folic acid increased from 28% in 1995 to 34% in 2000, a 22% increase
(25). Although folic acid consumption behaviors lag behind knowledge/awareness,
both behavior and knowledge have increased substantially among women aged
18--45 years, perhaps indicating that awareness is a precursor to voluntary behavior
change
(25). Although PRAMS estimates on awareness are slightly higher than
those reported in the literature, they represent somewhat different populations.
The PRAMS survey collects data from women who have recently given birth to a
live-born infant, whereas the March of Dimes survey assessed awareness among
women aged 18--45 years who are capable of becoming pregnant.
The format of the questions used by different surveys could also contribute to
the differences observed in prevalence estimates. The March of Dimes survey used
an open-ended format to collect information regarding folic acid
knowledge/awareness. The PRAMS survey is intended to gauge general awareness, not a)
whether respondents know how much folic acid to take, b) whether they know that they
need folic acid before and during the earliest days of pregnancy, or c) when (i.e., before
or during pregnancy) they became aware of the importance of taking folic acid.
Another survey, the BRFSS survey, uses multiple choice questions that query
reproductive-aged women regarding the purpose of folic acid. For 1996--1997, the BRFSS
reported that approximately 35% of women recognized the "correct" answer from
four options (26).
The analysis of PRAMS data also indicated that gaps in folic acid awareness
exist among women who have had live births. Women from racial or ethnic
minorities, who had attained a high school education or less, who received later or no
prenatal care, and whose pregnancies were unintended were less likely to be aware of
the benefits of folic acid. Other national studies have also reported gaps in folic
acid awareness and consumption among low-income populations
(25). One reason for these gaps could be that message dissemination within the health-care system is
less likely to reach some women before pregnancy, and folic acid information
must compete with many other health messages. Further research on the reasons for
the gaps in folic acid awareness could offer opportunities to learn more regarding
the effect of socioeconomic status (including available resources) on
women's prepregnancy health and pregnancy intentions.
Data in this study indicated that no substantial differences in folic acid
awareness existed among women of different age groups, parity, type of insurance, or
WIC participation. Analysis also indicated that women whose health-care
providers discussed nutrition during pregnancy were more likely to know the benefits of
folic acid intake. Similarly, focus group research conducted by CDC reported that
health professionals had more opportunity to discuss folic acid with women who
were already pregnant (32). Although this education probably occurs too late to help
many women prevent neural tube defects in their current pregnancy, the information
could help them plan for future pregnancies. All reproductive-aged women,
including uninsured women, should be provided the opportunity to discuss proper
nutrition with their primary-care providers before conception.
In contrast to other studies, the research in this study is strengthened by its
large, population-based sample from recent live births and its ability to identify gaps
in women's awareness regarding the benefits of folic acid in preventing some
birth defects. Although this study will be useful for promoting specific targeted
efforts, several limitations exist. First, this research focuses on women's awareness, and
no behavior data were available to assess folic acid consumption. Other studies of
folic acid consumption have demonstrated a substantial gap between folic acid
awareness and consumption behavior (25). Second, data from PRAMS could be biased
because
its surveys are administered after the birth of an infant, creating a time lapse
since early pregnancy when women might have learned about folic acid. Third, the
format of the PRAMS survey does not measure whether respondents know how much
folic acid to take or that they need folic acid before and during the earliest days
of pregnancy.
Although this study only assessed women's awareness of folic acid, other
findings were reported. Some states had high rates of awareness overall, whereas others
are lagging behind, and some populations are more disadvantaged than others.
Healthy People 2010 objectives call for a 50% reduction in neural tube defect cases and
an increase in daily consumption of 0.4 mg of folic acid from a baseline of 21% in
the early 1990s to 80% by 2010 among nonpregnant women aged 15--44
years (Objectives 16-15 and 16-16) (15). Recent research indicates that red blood cell
folate levels have increased among reproductive-age women
(16--18), likely because of a) food fortification and b) increased folic acid awareness efforts coupled with
some voluntary increase in folic acid consumption. Whether this increase has resulted in
a reduction of neural tube defects is unknown because of the current status of
research and the lag time in obtaining reliable data.
The results of this study could be used to promote healthier pregnancies
by encouraging a) more prepregnancy planning, b) greater consumption of diets rich
in vitamins (including folic acid) and minerals by women, and c)
increased preconceptional health education for all women of reproductive age. Given
the observed increase in women's awareness regarding folic acid over several
years, particularly after the implementation of major national and state efforts,
CDC recommends that health education efforts continue and expand on
multipronged strategies to reach women in low socioeconomic and cultural groups.
Specific messages and avenues of communication (e.g., media, interpersonal) for women
in racial and ethnic groups should be identified and mobilized. In addition,
health-care providers in general and prenatal-care providers in particular should take
advantage of every preconceptional and early prenatal encounter to educate women and
their families regarding pregnancy planning to ensure optimal pregnancy outcomes
for women and infants. Also, comprehensive reproductive health policies that
provide resources and opportunities for both men and women to make
optimal preconceptional decisions should be implemented by health-care providers.
Acknowledgements
We are grateful for the contributions of the PRAMS working group, which includes
the following states and collaborators: Albert Woolbright, Ph.D., Alabama; Kathy
Perham-Hester, M.S., Alaska; Gina Redford, M.A.P., Arkansas; Darci Cherry, M.P.H., Colorado; Richard
Hopkins, M.D., M.P.H., Florida; Tonya Johnson, Georgia; Barbara Yamashita, M.S.W., Hawaii;
Bruce Steiner, M.A., Illinois; Susanne Straif-Bourgeois, Ph.D., M.P.H., Louisiana; Martha
Henson, Maine; Donna Cheng, M.D., Maryland; Debbi Barnes-Josiah, Ph.D., Nebraska; Ssu Weng,
M.D., New Mexico; Ann Radigan-Garcia, New York State; Fabienne Laraque, M.D., New York
City; Paul Buescher, P.hD., North Carolina; Dick Lorenz, M.S., Oklahoma; Jo Bouchard, M.P.H.,
Ohio; Kristin Helms, M.S.P.H., South Carolina; Lois Bloebaum, Utah; Peggy Brozicevic, Vermont;
Linda Lohdefinck, Washington; Melissa Baker, M.A., West Virginia; and the CDC PRAMS team.
Kelley AE, Haddix AC, Scanlon KS, Helmick CG, Mulinare J. Cost-effectiveness of
strategies to prevent neural tube defects. In: Gold MR, Siegal JE, Russell LB, Weinstein MC, eds.
Cost effectiveness in health and medicine. New York, NY: Oxford University Press; 1996:313--48.
Laurence KM, James N, Miller MH, Tennant GB, Campbell H. Double-blind
randomised controlled trial of folate treatment before conception to prevent recurrence of
neural-tube defects. BMJ 1981;282:1509--11.
Mulinare J, Cordero JF, Erickson JD, Berry RJ. Periconceptional use of multivitamins and
the occurrence of neural tube defects. JAMA 1988;260:3141--5.
Milunsky A, Jick H, Jick SS, et al. Multivitamin/folic acid supplementation in early
pregnancy reduces the prevalence of neural tube defects. JAMA 1989;262:2847--52.
MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the
Medical Research Council Vitamin Study. Lancet 1991;338:131--7.
Czeizel AE, Dudas I. Prevention of the first occurrence of neural-tube defects
by periconceptional vitamin supplementation. N Engl J Med 1992;327:1832--5.
Shaw GM, Lammer EJ, Wasserman CR, O'Malley CD, Tolarva MM. Risks of orofacial clefts
in children born to women using multivitamins containing folic acid periconceptionally.
Lancet 1995;346:393--6.
Li DK, Daling JR, Mueller BA, Hickok DE, Fantel AG, Weiss NW. Periconceptional
multivitamin use in relation to the risk of congenital urinary tract anomalies. Epidemiology 1995;6:212--8.
Botto LD, Khoury MJ, Mulinare J, Erickson JD. Periconceptional multivitamin use and
the occurrence of conotruncal heart defects: results from a population-based, case-control
study. Pediatrics 1996;98:911--7.
US Food and Drug Administration. 21 CFR Parts 136, 137, and 139. Food
standards: amendment of standards of identity for enriched grain products to require addition of
folic acid. Federal Register 1996;61:8781--97.
Institute of Medicine. Dietary reference intakes: folate, other B vitamins, and choline.
In: Dietary reference intakes for thiamin, riboflavin, vitamin B6, folate, vitamin B12,
pantothenic acid, biotin & choline. Washington, DC: National Academy Press, 1998.
US Department of Health and Human Services. Healthy People 2010 (conference ed, 2
vols). Washington, DC: US Department of Health and Human Services, 2000.
Jacques PF, Selhub J, Bostom AG, Wilson PWF, Rosenberg IH. The effect of folic
acid fortification on plasma folate and total homocysteine concentrations. N Engl J
Med 1999;340:1449--54.
Lawrence JM, Petitti DB, Watkins M, Umekubo MA. Trends in serum folate after
food fortification [Letter]. Lancet 1999;354:915--6.
Scholl TO, Hediger ML, Schall JI, Khoo C-S, Fischer RL. Dietary and serum folate: their
influence on the outcome of pregnancy. Am J Clin Nutr 1996;63:520--5.
Locksmith G, Duff P. Preventing neural tube defects: the importance of periconceptional
folic acid supplements. Obstet Gynecol 1998;91:1027--34.
Rose NC, Mennuti MT. Periconceptional folic acid supplemention as a social
intervention. Semin Perinatol 1995;19:243--54.
Buehler JW, Mulinare J. Preventing neural tube defects. Pediatr Ann 1997;26:535--9.
Mulinare J. Public health perspective on folic acid and neural tube defects. Cereal
Foods World 1995;40:58--62.
March of Dimes. Folic acid and the prevention of birth defects. A national survey of
pre-pregnancy awareness and behavior among women of childbearing age.
1995--2000. Conducted by the Gallup Organization. White Plains, NY: March of Dimes, June
2000; publication no. 31-1404-00.
Broome KN, Mulinare J, Watkins ML. A comparison of reported folic acid usage and
knowledge among women of childbearing years (18--44) using BRFSS 1996 and 1997. In: Program
and abstracts of the 1999 Maternal, Infant, and Child Health Epidemiology Workshop:
building data capacity in maternal and child health. Atlanta, GA: US Department of Health and
Human Services, CDC, and Rockville, MD: Health Resources and Service Administration,
December 1999:155.
Colley Gilbert B, Shulman H, Fischer L, Rogers M. The Pregnancy Risk Assessment
Monitoring System (PRAMS): methods and 1996 response rates from 11 states. Matern Child Health
J 1999;3:199--209.
Hammond SL, Volansky M, Treiman K, Child W. Folic acid and birth defects prevention:
focus group research with women at risk. Rockville MD: Westat, Inc., July 1998; task no. 927650.
Daniel KL. Observations from the CDC: using health communications research to
reduce birth defects. J Women's Health 1999;8:19--22.
Henshaw SK. Unintended pregnancy in the United States. Fam Plann Perspect 1998;30:24--9.
Hammond SL, Cromer LC, Treiman K, Child W. Folic acid and birth defects prevention:
focus group research with health care providers. Rockville MD: Westat, Inc., July 1998; task
no. 927650.
* Alabama, Alaska, Arkansas, Colorado, Delaware, Florida, Georgia, Hawaii, Illinois,
Louisiana, Maine, Maryland, Mississippi, Nebraska, New Mexico, New York, North Carolina,
Ohio, Oklahoma, South Carolina, Utah, Vermont, Washington, and West Virginia.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.