National Vaccine Advisory Committee
Mary desVignes-Kendrick, M.D., Chair
City of Houston Department of Health
and Human Services
Houston, Texas
Amy Fine, Privacy and Confidentiality Chair
Health Policy/Program Consultant
Washington, D.C.
Marian Sokol, Ph.D., M.P.H., Resource Chair
Any Baby Can, Inc.
San Antonio, Texas
Patricia Whitley-Williams, M.D.,
Provider Chair
Robert Wood Johnson Medical School
New Brunswick, New Jersey
National Medical Association
Lorraine Cole, Ph.D.
National Medical Association
Washington, D.C.
Dennis Brooks, M.D.
Johnson Medical Center
Baltimore, Maryland
Council of State and Territorial Epidemiologists
Diane M. Simpson, M.D.
Texas Department of Health
Austin, Texas
Steve Waterman, M.D., M.P.H.
California State Department of Health Services
Berkeley, California
American Medical Informatics Association
Robert Jenders, M.D., Technology Chair
Columbia-Presbyterian Medical Center
New York, New York
Immunization Education Action Committee
Jack Blane, M.S.E.
Healthy Mothers, Healthy Babies
Highland Park, Illinois
Centers for Medicare and Medicaid Services
Rachael Block
Baltimore, Maryland
Department of Defense
Col. Renata Engler, M.D.
Walter Reed Army Hospital
Washington, D.C.
American Association of Health Plans
James E. Foy, D.O.
Kaiser Permanete
Powell, Ohio
Health Resources and Services Administration Rita M. Goodman, M.S.
Bethesda, Maryland
Partnership for Prevention
Christine M. Grant, M.B.A.
Swiftwater, Pennsylvania
National Association of County and City Health Officials Fernando A. Guerra, M.D., M.P.H.
San Antonio Metro Health District
San Antonio, Texas
City of Houston Health Department
Celine Hanson, M.D.
Houston, Texas
All Kids Count
Alan R. Hinman, M.D.
Task Force for Child Survival and Development
Decatur, Georgia
American Academy of Family Physicians
Leah Raye Mabry, M.D.
Pleasanton, Texas
U.S. Department of Agriculture and National Vaccine Advisory Committee
J. P. Passino, M.P.H.
Alexandria, Virginia
Pharmaceutical Research and Manufacturers of America
Lara Robillard
Washington, D.C.
Informed Parents Against VAPP (Vaccine-Associated Paralytic
Poliomyelitis) John B. Salamone
Oakton, Virginia
Inter-American College of Physicians
Luisa I. Sanchez, M.D.
New York, New York
Center for Health Information Management
Carla Marie Smith, M.A.
Ann Arbor, Michigan
Association of State and Territorial Health Officials F. E. Thompson, Jr., M.D.
Jackson, Mississippi
National Committee for Quality Assurance
Joseph W. Thompson, M.D., M.P.H.
Arkansas Children�s Hospital
Little Rock, Arkansas
American Academy of Pediatrics
Tomas Tonniges, M.D.
Elk Grove Village, Illinois
CDC Response to a Report from the National Vaccine
Advisory Committee
Summary
Immunization registries are confidential, population-based
computerized systems that contain information regarding children's vaccinations.
Registries provide a critical tool for increasing and sustaining vaccination coverage.
A national health objective for 2010 is to increase to 95% the proportion
of children aged <6 years who participate in fully operational
population-based immunization registries. According to 2000 data, 24% of U.S. children
are participating in population-based immunization registries. In 1998, to
facilitate community- and state-based immunization registry development in the
United States, the National Vaccine Advisory Committee (NVAC) launched the
Initiative on Immunization Registries. Through public hearings and parent focus
groups, NVAC identified four concerns that needed to be addressed to increase
registry participation: a) protecting each person's privacy and the confidentiality
of registry information; b) ensuring participation of vaccination providers
and recipients; c) overcoming technical and operational challenges; and
d) determining resources needed to develop and maintain immunization
registries. In January 1999, NVAC approved the report
Development of Community- and State-Based Immunization
Registries (available at
<http://www.cdc.gov/nip/registry/nvac.htm>; accessed July 30, 2001). The following report
summarizes NVAC's recommendations and describes CDC's National Immunization
Program activities in response to NVAC's recommendations.
BACKGROUND
Vaccinations are a critical public health tool: They save lives, reduce
health-care costs, and improve the quality of life for persons of all ages. After safe and
effective vaccines were introduced, the United States and the majority of other
developed countries have experienced >95% reductions in cases of childhood
vaccine-preventable diseases, compared with prevaccine-era levels
(1). Reported cases are at record low levels; however, vaccine-preventable diseases will return if
vaccination coverage levels decrease (2).
Reaching and Maintaining Increased Vaccination
Coverage Levels
Three successful strategies, implemented nationwide during the 1990s,
have boosted vaccination coverage to the highest levels ever
(3). These strategies include
reminder or recall systems maintained by health-care providers to notify
parents or guardians of preschool children of needed vaccinations;
the AFIX evaluation system implemented by public health departments
to Assess providers' vaccination coverage, provide
Feedback regarding results, provide
Incentives, and eXchange information to boost coverage and
avert missed vaccination opportunities; and
links between vaccination programs and the U.S. Department of
Agriculture's Special Supplemental Nutrition Program for Women, Infants, and Children
(WIC) to ensure that a child's immunization status is assessed at every WIC visit.
Maintaining increased vaccination coverage rates is a continuing challenge. In
the United States, an average of 11,000 infants are born daily, and each child
needs protection against vaccine-preventable diseases. Multiple factors threaten
continuing success, as follows:
New vaccines continue to be added to the already complex vaccination
schedule. Approximately 16--20 vaccine doses are recommended by age 18 months
(4). In addition, new vaccines and new combinations of vaccines will probably
become available (5).
In our increasingly mobile society, families relocate and change
medical providers or health insurance coverage with increasing frequency. This
mobility leaves medical and vaccination records scattered among different
caregivers, clinics, and offices, and results in incomplete records, unnecessary
vaccinations, or missed opportunities for vaccination administration
(6--10).
A limited number of providers use reminder or recall systems that notify
parents or guardians when their children need vaccinations
(11,12).
Both parents and providers overestimate vaccination coverage
(13--15).
Because the percentage of the population who receive vaccinations from
private providers has increased, the public health infrastructure designed to
administer vaccinations has declined (16).
Vaccine-preventable diseases are at record low levels; hence,
disease occurrence no longer reminds patients and providers of the need
for vaccinations.
Together, these factors cause difficulty for parents and providers in determining
a child's immunization status and ensuring that each child gets needed
vaccinations. Families, providers, and schools need definitive documentation of
childhood vaccinations, and communities and public health programs require accurate
coverage estimates. Community- and state-based immunization registries are a critical tool
for increasing and sustaining vaccination coverage; therefore, one Healthy People
2010 objective is to increase to 95% the proportion of children aged <6 years
who participate in fully operational, population-based immunization registries
(17).
INTRODUCTION
What Are Immunization Registries?*
Immunization registries are confidential, population-based, computerized
systems for maintaining information regarding children's vaccinations. A
population-based registry includes the majority of children in a geographic area, regardless of
health-care source. Children's names can be entered into the registry at birth (e.g., through
a link with electronic birth records) or at first contact with the health-care system. If
a registry includes all children in a geographic area and all providers report
vaccination and immunization data, the registry can provide a single data source for all
community vaccination partners. Registries enable implementing vaccination strategies, and
they decrease resources needed to measure, achieve, and maintain increased levels
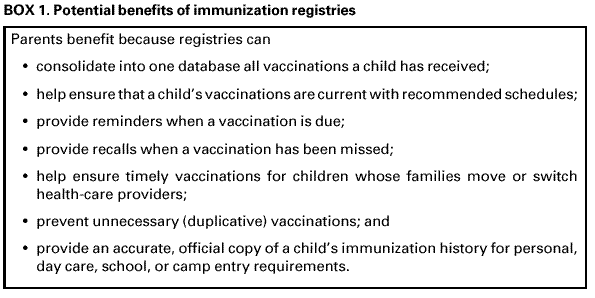
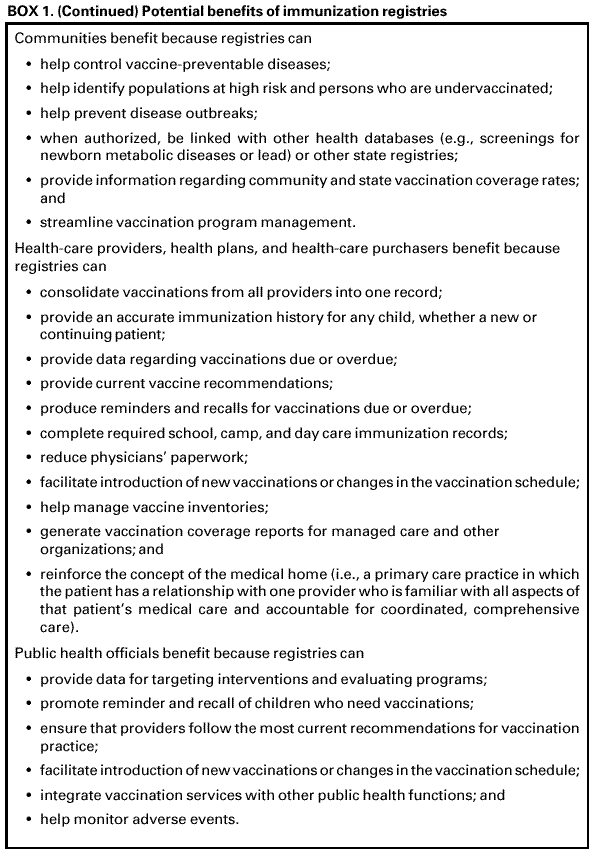
of vaccination coverage. Immunization registries offer potential benefits to
parents, communities, health-care systems, and the public health system (Box 1).
Efforts to Build U.S. Immunization Registries
In 1993, CDC began awarding planning grants to develop immunization registries
in every state. These systems were intended to collect immunization histories on
all children residing in the states. In 1994, NVAC's Subcommittee on
Vaccination Registries recommended expanded funding and new federal policies for a system
of immunization registries to support national goals. Since 1994, CDC has
allocated $181.3 million for the development and implementation of a nationwide network
of community- and state-based immunization registries to its 64 immunization
grantees (i.e., 50 states, the District of Columbia, Chicago, Houston, New York City,
Philadelphia, San Antonio, American Samoa, Guam, Marshall Islands, Micronesia, Northern
Mariana Islands, Palau, Puerto Rico, and the U.S. Virgin Islands) that receive federal
vaccination funds under section 317 of the Public Health Service Act. Private foundations have
also contributed funds for immunization registry development, including approximately
$20 million from the Robert Wood Johnson Foundation.
As of December 2000, a total of 39 (61%) of 64 grantees reported
operating population-based immunization registries that targeted their entire catchment
areas, and an additional 25 (39%) grantees reported developing
population-based immunization registries. In 2000, an estimated 24% of children aged
<5 years participated in a population-based immunization registry (CDC, unpublished
data, 2001).
NVAC's Initiative on Immunization Registries
In 1998, NVAC launched the Initiative on Immunization Registries to
facilitate community- and state-based immunization registry development in the United
States. Through public hearings and parent focus groups, NVAC's members and consultants
to the Initiative on Immunization Registries identified four challenges that needed to
be addressed to increase registry participation and to provide a framework for
their recommendations:
Protecting each person's privacy and the confidentiality of registry
information. Public health practitioners must consider each person's autonomy,
including privacy, confidentiality, and consent. In developing immunization registries,
these concerns become complex challenges. One difficult challenge is balancing
the need to gather and share immunization information with the need to
protect patients' and families' privacy.
Ensuring participation of vaccination providers and
recipients. Registries will be most useful if they have active participation from the majority of public
and private vaccination providers. Private provider adoption of systems has been
a slow process. Because of the shift in vaccination delivery from the public to
the private sector, registry projects need to enhance efforts to recruit
private providers. Educating recipients regarding the benefits of immunization
registries should encourage their participation. Recipient demand for registries
should encourage providers to participate.
Overcoming technical and operational
challenges. State and local communities have developed multiple systems that cover different jurisdictions, operate
in different hardware and software environments, use different software
packages, and vary in functionality. These systems should collect complete
immunization information regarding children and securely exchange this information
with other immunization registries, when appropriate.
Determining resources needed to develop and maintain
immunization registries. Information is needed regarding the initial and long-term costs
of developing and implementing registries, their cost-effectiveness, and
the consequences and costs of not developing registries. Sustainable
funding sources, which are based on that information, need to be identified.
In January 1999, NVAC approved the report resulting from the Initiative
on Immunization Registries (18). The following sections summarize
NVAC's recommendations and CDC's National Immunization Program activities in response
to those recommendations.
RECOMMENDATIONS AND CDC ACTIVITIES
Protecting Privacy and Confidentiality
NVAC Recommendations
Protecting privacy and maintaining confidentiality are essential to
developing immunization registries. Moreover, registry developers must consider
privacy and confidentiality concerns in light of their communities' values and
special needs.
The privacy and confidentiality concerns of immigrant communities must
be considered.
Federal legislation is needed to establish minimum privacy and
confidentiality standards. Moreover, the federal government should work with
key stakeholders, including NVAC, CDC, and the National Committee on Vital
and Health Statistics, to develop and disseminate model policies and legislation
for registries that enable exchanging information while protecting privacy
and confidentiality.
At a minimum, registry developers and operators should
--- ensure that patients and parents are notified of the existence of the
registry and of the information contained in the registry;
--- inform patients and parents of the registry's purpose and potential uses;
--- permit patients and parents to review and amend registry information; and
--- accept responsibility for registry information protection and reliability.
Parents must be given the option to decide whether their children will
participate in a registry. In certain communities, parents are informed of the registry,
its purposes, and potential uses during routine educational sessions offered at
the birth hospital. During such education sessions, or at any later time,
parents should be allowed to opt out of a registry. In communities where explicit
consent is preferred, the opting in or informed consent approach should be
offered. Parents should never be penalized for not participating in a registry.
Registry developers should limit access to registry information and
maintain audit trails to monitor records access. Each person should have access to his
or her own records and to audit trails.
Strong penalties for the unauthorized use of registry data should be in place
and consistently enforced.
Using registry data in a punitive manner against parents or patients (e.g.,
denial of health insurance coverage; U.S. Department of Justice, Immigration
and Naturalization Service tracking of immigrants; or other law
enforcement purposes) must be prohibited.
If registries are to be integrated with more substantial health
information systems, protecting privacy and confidentiality must be ensured.
The government should support an ongoing independent assessment of
the benefits, risks, and costs of registry development and implementation
with regard to privacy and confidentiality concerns.
CDC Activities
In response to these recommendations, a CDC-led Privacy and
Confidentiality Implementation Team with representatives from the National Vaccine Program
Office (NVPO), state health departments, and the All Kids Count (AKC) program,
developed minimum specifications for protecting the privacy of registry participants and
the confidentiality of registry data. Their report was reviewed by privacy consultants
and other stakeholders and approved by NVAC in February 2000
(19).
The specifications are based on the following principles:
An immunization registry is a tool for monitoring and improving
population-based health and personal health. The information contained in the
registry provides vaccination decision support. Registries do not replace parental
or provider responsibility.
Protecting privacy and maintaining confidentiality are essential to
successfully developing immunization registries.
Confidentiality policies are designed to balance clinical and public
health information needs with personal privacy rights.
Confidentiality policies are based on fair information practice, including
each person's right to know what information regarding him or her is in a record
and how it might be used and to request amendments or corrections to that record.
Deciding whether to participate in a registry and deciding whether to
vaccinate are separate decisions.
All immunization registries, including registries that are part of
integrated information systems, must ensure privacy protection.
Minimum specifications include, but are not limited to, the following:
Confidentiality
policies. All immunization registries must have a
written confidentiality policy that is consistent with applicable laws and applies
to everyone who has registry access.
Agreements to protect
confidentiality. All authorized registry users must sign
an agreement indicating that they understand the terms of the confidentiality
policy, including the penalties for violations, and that they agree to comply with
that policy. An employer can sign the agreement indicating that he or she
is responsible for the actions of his or her staff.
Notification. Patients or their parents or legal guardians must be notified of
the registry's existence, what information will be contained in it, how the
information will be used, with whom the information will be shared, the procedures
for review and correction of information, and how to exercise choice
regarding participation.
Choice. Parents must be able to choose whether to participate in the registry
and to change their decision at any time. Parents and children must not be
penalized for not participating. Personally identifiable information of those who
have chosen not to participate must be protected.
Use of immunization registry
information. Each registry must identify the purposes for which it collects immunization information and inform all
authorized users and parents or guardians. Information in the registry must only be used
for the purposes for which it was collected.
Access to and disclosure of immunization registry
information. Policies must define who will have access to registry information and specify to
which information those persons will have access. Policies must ensure that
only authorized users can provide information to or receive information from
the registry and that procedures are in place for handling requests from persons
and organizations that are not authorized users.
Penalties for unauthorized
disclosures. Policies must define what constitutes
a breach of confidentiality and delineate the legal and administrative policies
for the inappropriate use or disclosure of information. Penalties must be enforced.
Data retention and
disposal. Policies must address the amount of time
the information will be held in the registry and whether it will be deleted or
archived at the end of that period. Registries must have a written policy that provides
for the storage and disposal of all forms of confidential records.
Reports from states indicate that confidentiality policies are being developed
or modified to be consistent with these specifications. CDC continues to provide
technical assistance to states regarding these specifications. Additionally, CDC will assess
how well the minimum specifications apply to more substantial, integrated
information systems and to data sharing between managed care organizations and registries.
CDC and its partners will also explore other privacy concerns, including whether
persons reaching age 18 years should be notified that they are in the registry or that
their information is being archived.
As registries mature, interstate exchange of immunization information will
become more critical. Presently, inconsistent state laws control interstate information
sharing. States with stringent legal protections might not allow disclosure to states with
less protective laws. Therefore, CDC is facilitating guidelines development for
the interstate exchange of information.
Ensuring Participation of Vaccination Providers and Recipients
NVAC Recommendations
Providers and interested community groups should be involved
throughout registry development and implementation, beginning with the initial
planning stages.
Registries should be simple to use and designed to minimize the
administrative burden on vaccination providers. When possible, registries should capitalize
on data that providers already collect for billing or other purposes, thereby
avoiding duplicate data entry. This can be done by using billing or encounter
information systems, although modifications might be necessary to ensure
data completeness and quality. Initial and subsequent training should be provided
to
assist with the technical and administrative challenges associated
with seamlessly integrating registry functions into office environments.
Registries should include reminder or recall functions to improve adherence
to recommended vaccination schedules.
Data in immunization registries should be used to improve vaccination
services and coverage; these data should not be used to punish providers
whose vaccination coverage is below average.
CDC Activities
In 1997, to increase registry participation, CDC funded research projects to
a) identify strategies to encourage provider participation; b) improve registry data
quality by developing generalizable algorithms that ensure only one record per child in
a database; and c) assess the feasibility of avoiding duplicate data entry in
provider offices by enabling preexisting billing or patient management systems to
report vaccinations directly to an immunization registry.
Among the lessons learned from these projects is that provider
participation depends, in part, on high quality registry data. Registries must be able to
detect whether incoming information is already in the registry or is new. The majority
of registries have developed processes for detecting when a registry contains
multiple records for one child. Although no national criteria exist for evaluating
the effectiveness of registry duplication-reduction algorithms, efforts are on-going
to develop suitable evaluation criteria for these algorithms.
CDC is also developing a computerized tool that can examine registry
data accuracy and completeness by comparing registry records with vaccination
provider records. Furthermore, CDC is evaluating the feasibility of comparing
coverage estimates generated from the National Immunization Survey (NIS), which is
a nationwide, random-digit--dial survey of children's vaccination coverage in the
United States, with estimates based on registry databases. Concordance rates
between registry estimates and established standard estimates should reflect the
completeness and accuracy of immunization histories recorded in a registry's database.
Increased concordance rates should persuade providers and parents that registry data are
of high quality.
CDC has also identified registries that collect timely and complete
immunization information for a substantial proportion of their target population or a subgroup
of their population. Vaccination coverage estimates from these sentinel sites
are reported quarterly to CDC and compared with NIS estimates. These sites have
been used to monitor new vaccination recommendation implementation and to
demonstrate registry data usefulness in focusing public health interventions.
Even when immunization records are of high quality, making
appropriate vaccination decisions is difficult because of the complexity of vaccination schedules.
In 1995, CDC released its Programmer's Guide to the Automated
Immunization Evaluation Process, which offered assistance in developing automated
decision support algorithms that assess a child's immunization history and determine
which vaccinations are needed (20). Subsequently, algorithms were created
and incorporated into registries. To evaluate those algorithms, test cases were
developed,
and a public domain algorithm program that can function on multiple
computer platforms is available.**
CDC is establishing the Provider Participation Team and Work Group to
identify concerns and implement solutions to ensure participation of vaccination providers
and recipients in immunization registries. Initially, a national survey of pediatricians will
be conducted to understand what they think about immunization registries and
what would ensure their participation. Then, state vaccination projects will be surveyed
to identify current activities to recruit providers and determine best practices.
Ensuring Registry Functionality
NVAC Recommendations
CDC, in cooperation with state and local health agencies, provider
groups, software and hardware vendors, and national standard-setting
organizations, should lead the development, implementation, and maintenance of
standards pertaining to immunization registries, including
--- defining essential registry system functions and attributes;
--- defining core data elements;
--- certifying clinical decision-support functions;
--- certifying the registry's ability to consolidate multiple records of the same
person;
--- enabling intra- and interregistry record exchange with standard messages;
--- adopting system security standards to address technical and
administrative problems and to ensure that access is limited to authorized persons; and
--- certifying registry functions.
The initial target group for inclusion in immunization registries should be
children aged birth--<6 years, although registries might need to continue beyond
school entry or include other age groups (e.g., adolescents or older adults).
CDC Activities
In 1994, before these recommendations were made, CDC distributed the
first comprehensive description of the general structure and function of an
electronic immunization registry. At approximately the same time, CDC, in consultation
with immunization grantees and NVAC, also developed essential data elements to identify
a person and describe a vaccination event for record exchange. Core data
elements include a) patient name (first, middle, and last); b) patient birth date; c) patient sex;
d) patient birth state or country; e) mother's name (first, middle, last, and maiden);
f) vaccine type; g) vaccine manufacturer; h) vaccination or immunization date; and
i) vaccine lot number.
In 1997, because registries were being developed with different capabilities
and designs, CDC, in collaboration with immunization program managers, identified
the following 12 essential functions for immunization registries to be fully operational:
electronically store data for all NVAC-approved core data elements;
establish a registry record within 6 weeks of birth for each child in
the geographic catchment area;
enable access to and retrieval of immunization information in the registry at
each health-care encounter;
receive and process immunization information within 1 month of
vaccine administration;
protect the confidentiality of medical information;
ensure the security of medical information;
exchange immunization records by using the Health Level Seven
Organization (HL7)*** standard (21,22);
automatically determine which routine childhood vaccinations are needed,
in compliance with recommendations of the Advisory Committee on
Immunization Practices, each time a patient visits the health-care facility for a
scheduled vaccination;
automatically identify persons due or late for vaccinations to enable
production of reminder or recall notifications;
automatically produce vaccination coverage reports by provider, age group,
and geographic area;
produce official immunization records; and
promote accuracy and completeness of registry data.
In 1999, at the recommendation of NVAC, a technical working group (TWG),
which included external registry stakeholders and information technology specialists,
was formed. The purpose of the group was to a) reach agreement on
standard vocabularies and protocols for data transfer; b) serve as consultants to CDC
and recommend registry functional standards; c) assist in determining a
registry accreditation or certification method and provide ongoing quality
assurance monitoring; and d) indicate ways to facilitate the integration of registry functions
into existing information systems. Initial TWG accomplishments were their review
and agreement with the proposed functional standards, their development of
detailed definitions for these standards, and their identification of a method to certify
registries on the basis of these standards.
Progress has also been made in enabling registries to exchange data by
using standard coding and transmission rules defined by the HL7 standard
(21,22). In 1995, CDC began developing the standard HL7 immunization messages and
an
implementation guide for immunization record transactions. These messages
became a part of the final, balloted HL7 standard in 1997. In 2000, CDC received funding
from NVPO to develop a computer application that performs HL7 message functions.
Plans include placing this application in the public domain so that each registry
developer does not have to develop an application independently.
The technical focus of CDC's registry activities is related to identifying methods
to ensure reaching the 2010 health objective. CDC is reviewing measurable criteria
that have been proposed for each of the 12 functional standards. Standardized site
visit protocols addressing these elements were developed to monitor registry progress
in achieving the 2010 health objective relating to registries.
Ensuring Sustainable Registry Funding
NVAC Recommendations
CDC should further study registry start-up and maintenance costs and
compare these costs with those of alternative systems. Prospects for state and
local health agencies securing funds to support their immunization registries
should also be evaluated.
NVPO should coordinate discussions regarding recommendations for
long-term registry funding mechanisms.
A short-term (e.g., 3--5 year) federal appropriation should be sought to
support further registry development and initial implementation, with cost and
benefit analyses integral to these efforts. This funding would provide time to establish
a mechanism for long-term funding.
CDC Activities
Limited information is available regarding immunization registry costs. An
AKC study of 16 immunization registry projects in 1997 estimated that the cost
of maintaining immunization registries was approximately $3.91/child/year,
or approximately $94 million/year nationally to enroll all children aged <6 years
and keep them in the registry to age 6 years
(23). Similarly, a 1998 CDC study of three registries estimated an average annual cost of $3.38--$6.15/child/year, or
national costs of $81.1--$147.6 million/year. Additional 1999 CDC-collected data from
24 registries estimated an annual cost of $5.18/child, and an annual national cost
of $124.3 million. This study also determined that only 40% of registry costs were
funded by federal sources.
Registries offer potential cost savings. Estimated annual fiscal savings of
>$270 million associated with registries include costs of manually pulling medical records
in provider offices for school or day care entry ($58.0 million); costs of manually
pulling medical records in provider offices for changes in primary providers ($16.2
million); costs of duplicative vaccination ($26.5 million); costs of pulling records to
fulfill managed care reporting requirements ($2 million); and school system review
of
immunization records ($168.0 million)
(24--26). Registries might also reduce or
offset costs by reducing vaccine-preventable disease morbidity and mortality
through improved coverage, providing a means for assessing coverage at the local level,
and decreasing the incidence of vaccine adverse events through the identification
of children who have vaccine contraindications.
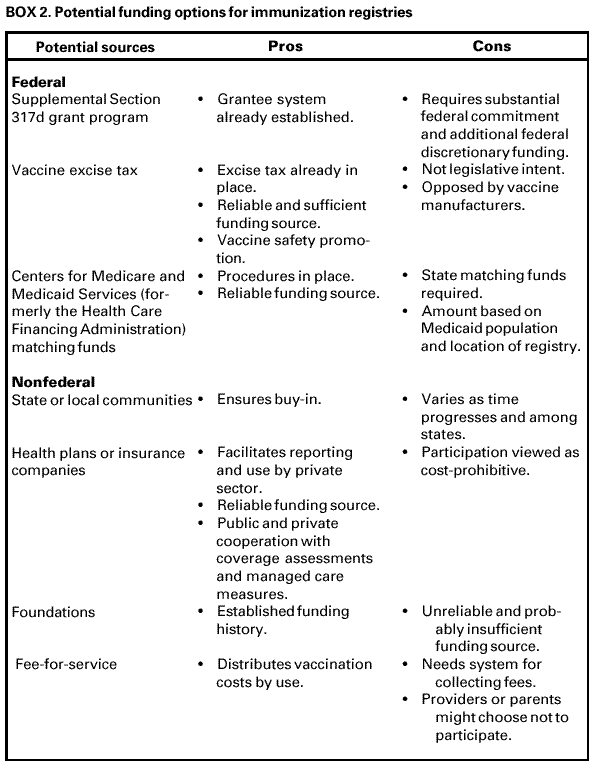
Involvement of all stakeholders in considering funding sources for registries will
be critical (Box 2). In 2000, the Centers for Medicare and Medicaid Services (formerly
the Health Care Financing Administration) agreed to fund approximately 90% of
registry development costs for Medicaid recipients. Although certain states have taken
this funding opportunity, other sources need to be identified for a long-term
funding solution.
OTHER REGISTRY-RELATED CONCERNS
Despite potential benefits of registries to vaccination coverage,
program operations, cost-savings, and parental support, immunization registries have
critics and opponents. In 1994, a congressional initiative to establish
population-based immunization registries throughout the country was proposed. Opponents
successfully argued against establishing a national immunization information
database. Consequently, efforts to establish state- and community-based immunization
registries were begun and have since resulted in the development of state and local
registries with different capabilities, legal authority, and success.
Concerns regarding immunization registries and their recommended uses
remain, including
ensuring registry participation by all or approximately all vaccination providers;
changing vaccination provider practices to rely on registry information
for coverage and programmatic data for improving vaccination services among
a population;
developing and applying a standard evaluation protocol to document that
each registry meets operational standards;
facilitating data flow from provider settings and local population-based
registries into and between state-based systems via the implementation of
nationally recognized data standards;
the implications of including data regarding a child's vaccine-associated
adverse events or contraindications to specific vaccines in a registry's database; and
appropriateness of integrating immunization data with other
childhood preventive health service information systems (e.g., blood lead screening
or newborn screening for metabolic abnormalities).
CONCLUSION
Population-based immunization registries, which collect information
regarding children within a specified geographic area, can be an effective means for
ensuring
that children remain current with recommended vaccination schedules.
Additionally, registries allow programs to rapidly and completely assess vaccination coverage
in defined areas or among specific groups of children. Despite their
advantages, registries have developed slowly, and only a limited number of registries are close
to meeting the Healthy People 2010 national objective of increasing to 95%
the proportion of children aged <6 years who participate in fully operational
population-based immunization registries.
In 1998, NVAC held public hearings that produced four recommendations
for immunization registries: a) ensure each person's privacy and the confidentially of
the information collected; b) ensure participation by all vaccination providers
and recipients; c) ensure functionality; and d) ensure sustainable funding. CDC has
worked on each of these recommendations with its partners. Minimum specifications
to protect privacy and confidentiality have been developed and approved by NVAC. A
set of 12 minimum operational standards have been established for
population-based immunization registries, and standardized evaluation criteria to monitor
registry progress are being developed. The Centers for Medicare and Medicaid Services
plans to share the financial burden of state registries. Although these actions do
not guarantee that state and local vaccination programs can develop and implement
fully operational registries, this national approach to standardization and shared
allocation of substantial resources will facilitate this process.
Ensuring participation by all providers and recipients has been more difficult and
is not yet close to achievement. Survey data in 2000 estimate that, nationwide, only
24% of children aged <6 years are participating in an immunization registry
(CDC, unpublished data, 2001). Although certain national organizations have
formally supported the concept of immunization registries, practitioners still find
routine participation difficult to implement. Overcoming barriers to full participation
remains the greatest challenge to population-based immunization registries.
References****
1. Orenstein WA, Hinman AR, Rodewald LE. Public health considerationsCUnited
States [Chapter 42]. In: Plotkin SA, Orenstein WA. Vaccines. Philadelphia, PA: W.B.
Saunders Co., 1999;1023.
2. Gangarosa EJ, Galazka AM, Wolfe CR, et al. Impact of anti-vaccine movements
on pertussis control: the untold story. Lancet 1998;351:356--61.
3. Shefer A, Briss P, Rodewald L, et al. Improving immunization coverage rates:
an evidence-based review of the literature. Epidemiol Rev 1999;21:96--142.
5. Committee on Immunization Finance Policies and Practices, Division of Health
Care Services and Division of Health Promotion and Disease Prevention, Institute
of Medicine. Building, monitoring, and sustaining immunization capacity [Chapter 4].
In: Calling the shots: immunization finance policies and practices. Washington,
DC: National Academy Press, 2000;103--41.
6. Hamlin JS, Wood D, Pereyra M, Grabowsky M. Inappropriately timed
immunizations: types, causes, and their relationship to record keeping. Am J Public Health
1996;86: 1812--4.
7. Ortega AN, Andrews SF, Katz SH, et al. Comparing a computer-based
childhood vaccination registry with parental vaccination cards: a population-based study
of Delaware children. Clin Pediatr 1997;36:217--21.
8. Szilagyi PG, Rodewald LE, Humiston SG, et al. Missed opportunities for
childhood vaccinations in office practices and the effect on vaccination status.
Pediatrics 1993;91:1--7. Erratum: Pediatrics 1993;91:545.
9. Watson MA, Feldman KW, Sugar NF, Sommer CJ, Thomas ER, Lin T. Inadequate
history as a barrier to immunization. Arch Pediatr Adolesc Med 1996;150:135--9.
10. Murphy TV, Pastor P, Medley FB. Factors associated with unnecessary
immunization given to children. Pediatr Infect Dis J 1997;16:47--52.
11. Lieu TA, Black SB, Ray P, et al. Computer-generated recall letters for
underimmunized children: how cost-effective? Pediatr Infect Dis J 1997;16:28--33.
13. Bushnell CJ. ABC's of practice-based immunization assessments. In:
28th National Immunization Conference Proceedings, Charlotte, North Carolina, June 13--17,
1994. Atlanta, GA: US Department of Health and Human Services, Public Health Service,
CDC, 1994:207--9.
14. Goldstein KP, Kviz FL, Daum RS. Accuracy of immunization histories provided by
adults accompanying preschool children to a pediatric emergency department.
JAMA 1993;270:2190--4.
15. Joffe MD, Luberti A. Effect of emergency department immunization on
compliance with primary care. Pediatr Emerg Care 1994;10:317--9.
16. Szilagi PG, Humiston SG, Shone LP, Barth R, Kolasa MS, Rodewald LE. Impact
of vaccine financing on vaccinations delivered by public health clinics. Am J
Public Health 2000;90;739--45.
17. US Department of Health and Human Services. Healthy people 2010 (conference ed,
vol 1). Washington, DC: US Department of Health and Human Services, 2000. Available
at <http://www.health.gov/healthypeople>. Accessed July 30, 2001.
18. National Vaccine Advisory Committee (NVAC). Development of community and
state-based immunization registries; approved January 12, 1999. Atlanta, GA: US
Department of Health and Human Services, CDC, 1999. Available at
<http://www.cdc.gov/nip/registry/nvac.htm>. Accessed July 30, 2001.
19. All Kids Count Program of the Task Force for Child Survival and Development and
the National Immunization Program of CDC. Chapter II: Confidentiality. In:
Community immunization registries manual. Atlanta, GA: US Department of Health and
Human Services, CDC, 2000; II-1--II-39. Available at
<http://www.cdc.gov/nip/registry/dl/cirman2.pdf>. Accessed July 30, 2001.
20. CDC. Programmer's guide to the automated immunization evaluation process,
version 2.0, March 31, 2000. Atlanta, GA: Department of Health and Human Services,
CDC, National Immunization Program. Available at
<http://www.cdc.gov/nip/registry/peg.pdf>. Accessed August 9, 2001.
21. CDC. Implementation guide for immunization data transactions using version 2.3.1
of the Health Level Seven (HL7) standard protocol: implementation guide version
2.0, June 1999. Atlanta, GA: Department of Health and Human Services, CDC,
National Immunization Program. Available at <http://www.cdc.gov/nip/registry/hl7guide.pdf>.
Accessed August 9, 2001.
22. Health Level Seven, Inc. Health Level Seven. Ann Arbor, MI: Health Level Seven,
Inc., 2001. Available at <http://www.hl7.org>. Accessed August 9, 2001.
23. Horne PR, Saarlas KN, Hinman AR. Costs of immunization registries: experiences
from the All Kids Count II projects. Am J Prev Med 2000;19:94--8.
24. All Kids Count. Sustaining financial support for immunization registries [Policy
brief]. Decatur, GA: All Kids Count, 2001. Available at <http://www.allkidscount.org>.
Accessed July 31, 2001.
25. Horne PR, Saarlas KN, Hinman AR. Update on immunization registries [Letter]. Am
J Prev Med 2001;20:174.
26. Feikema SM, Klevens RM, Washington ML, Barker L. Extraimmunization among
US children. JAMA 2000;283:1311--7.
*In addition to tracking the vaccinations children receive, fully operational
immunization registries can improve vaccine delivery by a) avoiding duplicate vaccinations, b)
limiting the cost of missed appointments through the use of reminder or recall notices,
c) reducing vaccine waste, and d) reducing staff time required to find or
produce immunization records or certificates. In certain regions, immunization registries
provide programs a rapid and reliable mechanism for evaluating their vaccination coverage
and patterns of use for specific vaccines. Also, registries can assist in vaccine safety
efforts and can be used for vaccine ordering and inventory control. Therefore, the
term immunization registry is used throughout this report, rather than
vaccination registry, to better reflect their capabilities.
**The algorithm program is available upon request by calling (404) 639-8739 or
by electronic mail at <CASAINFO@cdc.gov>.
***Health Level Seven (Ann Arbor, Michigan) is an American National Standards
Institute-accredited organization that develops specifications or protocols for health-care
data management. Additional information is available at <http://www.hl7.org> (accessed
July 30, 2001).
****All MMWR references are available on the Internet at
<http://www.cdc.gov/mmwr>. Use the search function to find specific articles.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.