|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
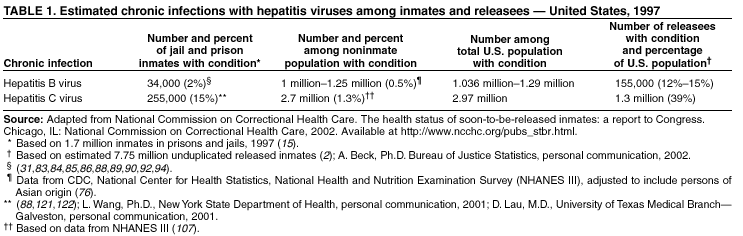
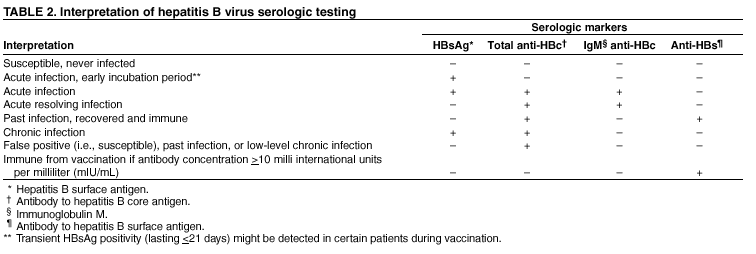
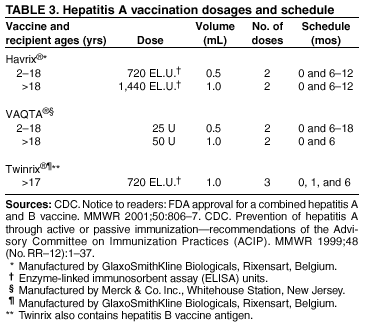
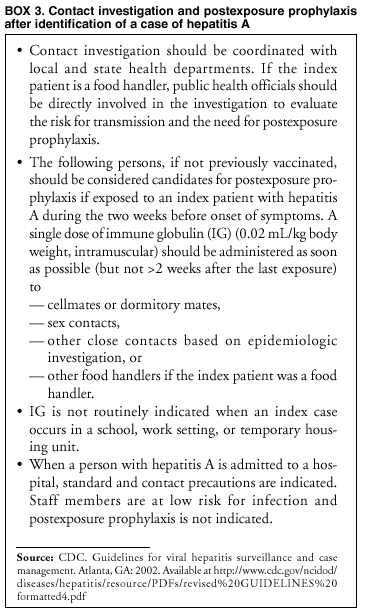
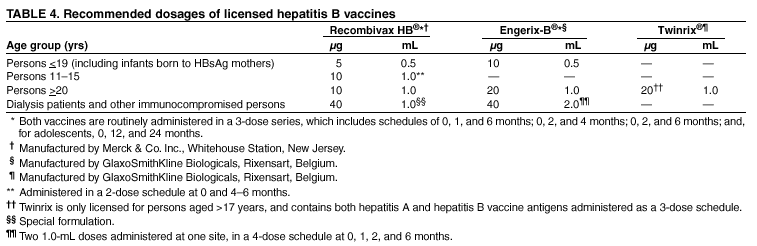
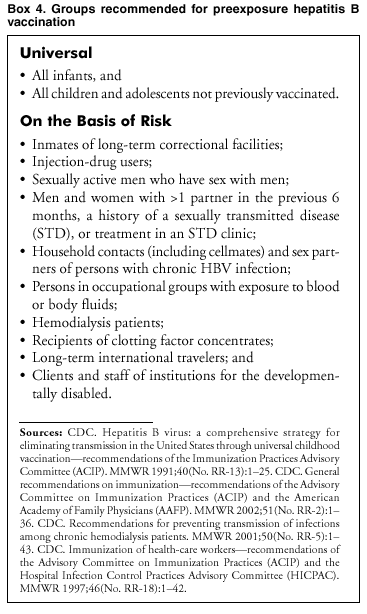
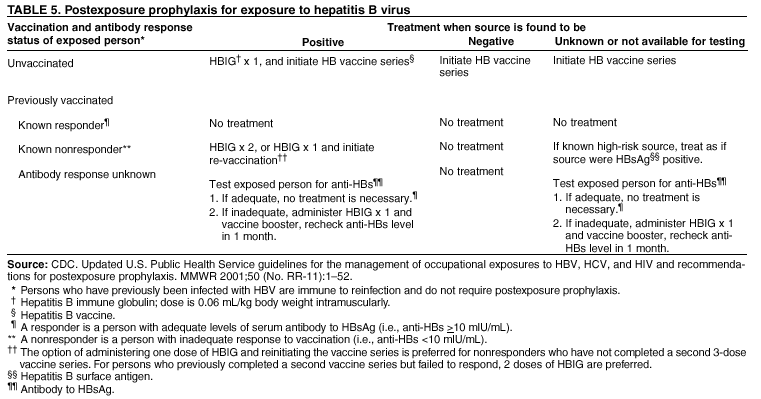
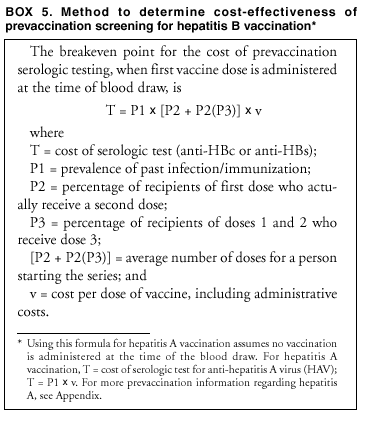
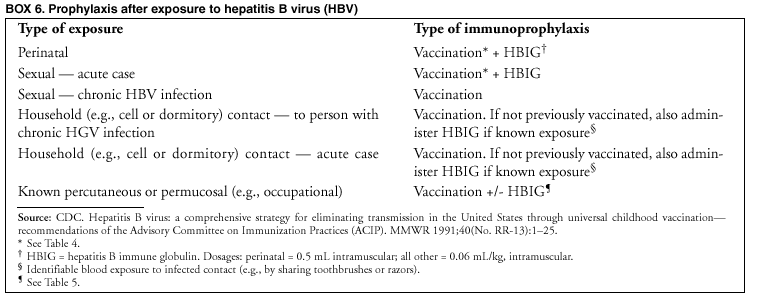
Prevention and Control of Infections with Hepatitis Viruses in Correctional SettingsPlease note: An erratum has been published for this article. To view the erratum, please click here. Prepared by The material in this report originated in the National Center for Infectious Diseases, James M. Hughes, M.D., Director, and the Division of Viral Hepatitis, Harold S. Margolis, M.D., Director. SummaryThis report consolidates previous recommendations and adds new ones for preventing and controlling infections with hepatitis viruses in correctional settings. These recommendations provide guidelines for juvenile and adult correctional systems regarding 1) identification and investigation of acute viral hepatitis; 2) preexposure and postexposure immunization for hepatitis A and hepatitis B; 3) prevention of hepatitis C virus infection and its consequences; 4) health education; and 5) release planning. Implementation of these recommendations can reduce transmission of infections with hepatitis viruses among adults at risk in both correctional facilities and the outside community. These recommendations were developed after consultation with other federal agencies and specialists in the fields of corrections, correctional health care, and public health at a meeting in Atlanta, March 5--7, 2001. This report can serve as a resource for those involved in planning and implementing health-care programs for incarcerated persons. IntroductionPersons incarcerated in correctional systems comprise approximately 0.7% of the U.S. population and have a disproportionately greater burden of infectious diseases, including infections with hepatitis viruses and other infections of public health importance (e.g., human immunodeficiency virus [HIV], sexually transmitted disease [STD], and tuberculosis [TB] infections) (1). In 2000, >8 million inmates of prisons and jails were released and returned to the community (A. Beck, Ph.D., Bureau of Justice Statistics, personal communication, 2002). Recent estimates indicate 12%--39% of all Americans with chronic hepatitis B virus (HBV) or hepatitis C virus (HCV) infections were releasees during the previous year (1) (Table 1). The significance of including incarcerated populations in community-based disease prevention and control strategies is now recognized by public health and correctional professionals (2,3). Improved access to medical care and prevention services for incarcerated populations can benefit communities by reducing disease transmission and medical costs (4--8). Inmates who participate in health-related programs while incarcerated have lower recidivism rates and are more likely to maintain health-conscious behaviors (4). Finally, because incarcerated persons have a high frequency of infection with hepatitis viruses, community efforts to prevent and control these infections require inclusion of the correctional population (9--11). However, implementation of preventive health programs for incarcerated persons has substantial challenges. Correctional staff are among groups at potential risk for occupationally acquired infections with bloodborne pathogens. Therefore, recommendations are also reviewed for prevention and control of infections with hepatitis viruses among correctional workers. Definitions Adolescent: Person aged >10 and <19 years. Anti-HBc: Antibody to hepatitis B core antigen; positive test indicates past or current infection with HBV. Anti-HBs: Antibody to hepatitis B surface antigen; indicates immunity to HBV infection, either from HBV infection or immunization. Anti-HCV: Antibody to HCV; positive test indicates past or current infection with HCV. Arrestee: Person placed under arrest by law enforcement who has not been formally charged with a crime. Body fluids, potentially infectious: Semen, vaginal secretions, cerebrospinal fluid, synovial fluid, pleural fluid, pericardial fluid, peritoneal fluid, and amniotic fluid. Potentially infectious body fluids include any body fluid visibly contaminated with blood, and all body fluids in situations where identifying blood contamination is difficult or impossible. Detainee: Person arrested and legally charged with a crime who is held in a correctional facility before trial. HAV: Hepatitis A virus, the infectious agent that causes HAV infection and hepatitis A. HBIG: Hepatitis B immune globulin; sterile preparation of high-titer antibodies (immunoglobulins) to hepatitis B surface antigen obtained from pooled human plasma of immunized persons and which provides protection against HBV infection. HBeAg: Hepatitis B e antigen; positive test correlates with HBV replication and infectivity. HBsAg: Hepatitis B surface antigen; positive test indicates an active HBV infection. HBV: Hepatitis B virus, the infectious agent that causes HBV infection, hepatitis B, and chronic liver disease. HBV DNA: Deoxyribonucleic acid from HBV; positive test indicates active infection. HCC: Hepatocellular carcinoma; a primary liver cancer caused by chronic HBV or HCV infection that is usually fatal. HCV: Hepatitis C virus, the infectious agent that causes HCV infection, hepatitis C, and chronic liver disease. HCV RNA: Ribonucleic acid from HCV; positive test indicates active infection. HDV: Hepatitis D virus, a viroid (incomplete virus) that requires an active (acute or chronic) HBV infection to replicate and cause delta hepatitis virus infection, delta hepatitis, and chronic liver disease. IDUs: Injection-drug users; persons who have ever used needles to inject illicit drugs. IgM anti-HAV: Immunoglobulin M antibody to HAV; positive test indicates acute HAV infection. IgM anti-HBc: Immunoglobulin M antibody to hepatitis B core antigen; positive test indicates acute HBV infection. IG: Immune globulin; sterile preparation of antibodies (immunoglobulins) made from pooled human plasma that contains anti-HAV and provides protection against hepatitis A. Infant: Person aged <1 year. Inmate: Incarcerated person. Jail: Locally operated correctional facility that confines persons pending arraignment, awaiting trial and sentencing, or serving their sentences (usually <1 year). Juvenile: Person aged <19 years, in custody of the legal system. Prison: Adult correctional facility under the jurisdiction of state or federal authorities that confines persons with a sentence of >1 year. Seroconversion: The change of a serologic test from negative to positive. Seroprotection: Level of antibodies necessary to protect against infection. Correctional PopulationsJuvenilesIn 1997, approximately 12% of persons aged 16 years reported at least one arrest in their lifetimes (12). In 1999, a reported 108,965 juvenile offenders were held in residential placement facilities (13). In 1994, the average length of stay in public facilities for juvenile releasees was 2 weeks for those detained and 5 months for those committed; the stay in private facilities (primarily a committed population) averaged 3.5 months (12). Of arrested juveniles not incarcerated, the majority are diverted to alternative programs (e.g., teen courts or restorative justice) where they remain under supervision of the juvenile justice system. Approximately 74% of incarcerated juvenile offenders are held in public facilities, and the rest in facilities operated by private contractors (14). Adult jails hold >7,600 juveniles, and approximately 3,100 are held in adult prisons (15). Females account for 27% of juveniles arrested and 13% of those in residential placement (14,16). Of juveniles arrested in 1999, approximately 72% were white, 25% black, and 3% of other races. However, a disproportionate number of racial and ethnic minorities were detained in residential placement (40% black and 18% Hispanic). AdultsAt the end of 2001, adult jail and prison populations totaled 1.96 million --- a 71% increase from 1990 (13). Prior incarceration as juveniles was reported by 9% of adults in federal prisons and by 20% in state prisons (17). According to 2000 data, racial/ethnic minorities were overrepresented, with 46% black, 36% white, 16% Hispanic, and 2% other races. Approximately 6.6% of adult inmates are female, a 111% increase since 1990; of incoming women to state prisons, 5% are pregnant (18). Among adult U.S. residents, 1 in every 112 men and 1 in every 1,724 women were sentenced to state or federal prisons in 2001 (13). The estimated 12.6 million admissions and 12.6 million releases from local jails, and 625,000 admissions and 606,000 releases from prisons represent annual turnover rates of 1300% and 40%, respectively (1,15; A. Beck, Ph.D., Bureau of Justice Statistics, personal communication, 2002). StaffIn 2000, >457,000 custody and security officers worked in the U.S. correctional system, including both public and private sectors (19). These officers comprise approximately two thirds of all correctional staff, which also includes professional, technical, educational, clerical, maintenance, food service, and administrative workers (20,21). Health Care in the Correctional SystemUpon incarceration, all adults and the majority of juveniles lose access to the usual public and private health-care and disease-prevention services. Their health care becomes the sole responsibility of either the correctional system (federal, tribal, state, or local), or less frequently, the public health system (22). For the majority of persons, entry into the correctional system provides an opportunity to access health care. In one series, approximately 78% of newly incarcerated females had abnormal Papanicolaou smears, and >50% had vaginal infections or STDs (23). However, the rapid turnover of the incarcerated population, especially in jails, and the suboptimal funding of correctional health and prevention services, often limits the correctional system in providing both curative and preventive care. Infectious diseases --- including acquired immune deficiency syndrome (AIDS), STDs, TB, and viral hepatitis --- are more prevalent among correctional inmates than the general population. In 1997, an estimated 46,000--76,000 prison and jail inmates had serologic evidence of syphilis; 8,900 had AIDS (4% of the U.S. AIDS burden); and 1,400 had active TB (4% of the U.S. TB burden) (1). Among incarcerated persons, shared risk factors (e.g., injection-drug use) can result in populations coinfected with HBV, HCV, or HIV. Coinfections can make treatment of chronic viral hepatitis, AIDS, and TB more difficult because of the need to use multiple drugs, which increases the chance of hepatotoxicity and other adverse events. In addition, both TB chemoprophylaxis and HIV postexposure prophylaxis can be complicated by the presence of chronic liver disease (24,25). Risk Factors for Viral Hepatitis Transmission Among Incarcerated PersonsDrug UseDuring 1990--1999, the rate of arrest for substance abuse violations among persons aged 10--17 years increased by 132% (12,26). Injection-drug use is reported by 3.3%--6% of incarcerated juveniles (A. Thomas, M.D., Oregon Health Division; and R. Bair, M.D., Bexar County Juvenile Detention Center, San Antonio, Texas; personal communications, 2001). Among juvenile detainees, 53% of males and 38% of females tested positive for marijuana use at the time of arrest, <17% tested positive for cocaine, and <18% were positive for methamphetamine (27). Arrested adults also have a high prevalence of illicit drug use. In 2000, 21% of state prisoners and 59% of federal prisoners were incarcerated for drug offenses (13). In 1997 inmate surveys, 83% of state prisoners and 73% of federal prisoners reported past drug use, and 57% of state prisoners and 45% of federal prisoners reported using drugs in the month before their offense (28). Among jail inmates, drug use in the month before incarceration was reported by 55%, and injection-drug use was reported by 18% (29). However, urine testing at entry has indicated drug use might be substantially underreported by jail inmates (30). Injection-drug use during incarceration has been reported by 3%--28% of adult inmates (31--34). Although certain correctional systems offer substance-abuse treatment and education programs, demand usually exceeds program capacity (20). There appear to be no comprehensive risk-reduction programs available within correctional facilities. Sexual BehaviorAll states have laws prohibiting sex between adult residents of correctional systems (35). Despite these laws, 2%--30% of inmates have sex while incarcerated (31,36--38). Outbreaks of syphilis and hepatitis B among inmates reflect sexual activity in correctional facilities (31,33,39,40). Although two state prison systems and five city or county correctional systems make condoms available to adult inmates and detainees for use in their facilities (Vermont, Mississippi, New York City, Philadelphia, San Francisco, Washington D.C., Los Angeles), no juvenile correctional systems are known to provide condoms (E. Dunlap, National Juvenile Detention Association, personal communication, 2001). Percutaneous Exposures of Uncertain RiskPercutaneous exposures have the potential to transfer infectious blood and transmit bloodborne pathogens. Tattoos and other percutaneous exposures (e.g., bites and abrasions) are common in correctional facilities and have the potential to expose residents and correctional staff to blood and body fluids (34,41,42). Case-control studies indicate tattooing is not a risk factor for acquiring acute hepatitis B or hepatitis C (43,44). However, results from seroprevalence studies of noninstitutionalized populations have been variable, and studies of highly select groups might not be generalizable to other populations (45). One study of a limited number of IDUs suggested an increased risk for both HBV and HCV infection among those tattooed while in prison (46), but limited studies of both adult and juvenile inmate populations have not confirmed this finding (33; R. Bair, M.D., Bexar County Juvenile Detention Center, San Antonio, Texas, personal communication, 2001). Occupational ExposuresCorrectional employees have reported injuries from human bites, needles, and other sharp instruments, as well as skin and mucous membrane exposures to blood and body fluids (41,42). Occupational transmission of HBV infection among hospital-based workers has been linked to percutaneous and mucous membrane exposures, and HBV infection has been primarily associated with percutaneous exposure. Transmissions of HBV and HCV infections have not been associated with intact skin exposures (10,47). Limited data from correctional workers have indicated 21% reported blood contact with intact skin, and 7% reported a percutaneous exposure (including needle stick, cut with a contaminated object, or bite) or mucus membrane exposure (48). Epidemiology and Outcome of Infection with Hepatitis VirusesHepatitis A Virus InfectionHAV infection is usually acquired by the fecal-oral route, produces a self-limited disease that does not result in chronic infection or long-term liver disease, and usually produces symptoms of acute viral hepatitis among adolescents and adults after an average incubation period of 28 days (range: 15--50 days). Signs and symptoms usually last <2 months, although 10%--15% of symptomatic persons have prolonged or relapsing disease lasting <6 months (49). Peak infectivity occurs during the 2-week period before the onset of jaundice or elevation of liver enzymes, when the concentration of virus in stool is highest (11). Persons with chronic liver disease who acquire hepatitis A are at increased risk for fulminant hepatitis (50). Epidemiology of HAV Infection In the United States, the majority of cases of hepatitis A occur through person-to-person transmission during communitywide outbreaks (11,51). Viral transmission can occur through close personal contact (e.g., household contact, sexual contact, drug use, or children playing), and contaminated food or water (e.g., infected food-handlers or raw shellfish). The most frequently reported source of infection (12%--26%) is household or sexual contact with a person with HAV infection; however, 45%--50% of patients have no identified source for their infection (51,52). Historically, the highest rates of disease have occurred in 11 western U.S. states and certain counties, which accounted for approximately 50% of cases during 1987--1997 (11,52). HAV infection is common among IDUs. Injection-drug use has been reported by 5%--19% of hepatitis A patients. In certain communities, hepatitis A outbreaks involving users of injected and noninjected methamphetamine have accounted for approximately 30% of reported cases (11,51,53,54). Cross-sectional serologic surveys demonstrate that users of illicit drugs have a higher prevalence of infection than the general U.S. population (11,55). Viremia occurs during HAV infection, and transmission has occurred from parenteral blood exposure (e.g., blood transfusion or injection-drug use) on occasion (56). However, the majority of transmissions among users of illicit drugs are believed to occur through fecal contamination of drug paraphernalia and subsequent percutaneous inoculation, as well as from close personal contact (57). Hepatitis A outbreaks among men who have sex with men (MSM) are frequently reported, and cyclic outbreaks occur in urban areas of the United States (58,59). HAV-infected MSM report more frequent oral-anal contact, longer duration of sexual activity, and a larger number of sex partners than persons without serologic evidence of infection (60--63). HAV Infection in Correctional Settings No hepatitis A outbreaks have been reported from correctional settings, although a substantial proportion of incarcerated persons have risk factors for infection (e.g., drug use or MSM). The prevalence of prior HAV infection among incarcerated persons is estimated at 22%--39%, which is similar to age-adjusted prevalence rates in the general U.S. population (11; C. Shapiro, M.D., CDC, personal communication, 2002; T. Lincoln, M.D., Hampden County Correctional Center, Ludlow, Massachusetts; and D. Lau, M.D., University of Texas Medical Branch---Galveston; personal communications, 2001). Employment in a correctional setting has not been identified as a risk factor for HAV infection. Hepatitis B Virus InfectionHBV is a bloodborne pathogen, transmitted by percutaneous or permucosal (e.g., sexual) exposure to infectious blood or body fluids (e.g., semen or saliva). HBV circulates in high titers in the blood and lower titers in other body fluids (e.g., semen, vaginal fluid, or saliva), and is approximately 100 times more infectious than HIV and 10 times more infectious than HCV (47). Acute hepatitis B develops in approximately 30%--50% of adults at the time of initial infection and is characterized by anorexia, nausea, vomiting, and often jaundice. The risk of progression to chronic infection varies with age, being highest among young children and infants (30%--90%) and lowest among adolescents and adults (2%--6%) (64). The majority of persons with chronic HBV infection are asymptomatic, and one third have no evidence of liver disease, despite high levels of viral replication in hepatocytes (65). The remainder have chronic hepatitis (mild, moderate, or severe) that can lead to cirrhosis and HCC. Persons with chronic HBV infection have a 15%--25% lifetime risk of death from chronic liver disease or HCC (66--70). Rates of progression to cirrhosis and HCC vary according to age at acquisition of chronic infection; HBeAg status; coinfection with HDV, HIV, HCV; and alcohol abuse (69,71--75). HBV-related liver disease and HCC cause approximately 3,000 deaths in the United States annually (S. Goldstein, M.D., CDC, unpublished data, 2002). Epidemiology of HBV Infection An estimated 5% of the civilian, noninstitutionalized U.S. population has serologic evidence of past or present HBV infection, and 0.4%--0.5% have chronic infection and serve as the primary source of infection for others (9,76). Overall prevalence of HBV infection differs among racial/ethnic populations and is highest among persons who have immigrated from areas with a high endemicity of HBV infection (e.g., Asia, Pacific Islands, Africa, and the Middle East) (77). Prevalence of infection among blacks is four times prevalence among whites (11.9% compared with 2.6%) (76). During 1987--1998, reported cases of acute hepatitis B declined by 76% (8). Nonetheless, an estimated 78,000 persons were infected with HBV in 2001 (G. Armstrong, M.D., CDC, unpublished data, 2002). Disease incidence is highest among blacks, followed by Hispanics and whites, and highest among persons aged 25--39 years (8,52). The age of newly infected persons has increased from a median of 27 years during 1982--1988 to 32 years during 1994--1998, probably as a result of vaccination of adolescents and young adults and changes in high-risk behaviors in certain populations (8). Before national prevention programs began in 1990, perinatal and early childhood transmission accounted for 30% of chronic HBV infections (78). Sex is the predominant mode of HBV transmission among adults and adolescents, accounting for more than half of newly acquired infections (8). Among reported cases of acute hepatitis B, approximately 40% reported heterosexual exposure to an infected partner or multiple partners, and 15% were MSM. In addition, 14% of persons with acute hepatitis B reported injection-drug use. Thirty-three percent of persons with acute hepatitis B cannot identify a risk factor for infection, although approximately 50% of those persons have a history of known risk factors (8). HBV Infection in Correctional Settings Juveniles. The majority of juvenile offenders have behaviors that place them at risk for HBV infection (e.g., injection-drug use or unprotected sex with multiple partners). The prevalence of past HBV infection among noninstitutionalized high-risk juveniles (e.g., homeless, drug-using, or HIV-positive) ranges from 3.6% to 19% (79--81) (B.M. Beech, Ph.D, University of Memphis, Tennessee, 2002), compared with the <3% prevalence of infection among adolescents in the general population (76,82). Among incarcerated juveniles, prevalence of past HBV infection ranges from 0% to 6% (79,82; A. Thomas, M.D., Oregon Health Division; and R. Bair, M.D., Bexar County Juvenile Detention Center, San Antonio, Texas; personal communications, 2001). HBV transmission has not been observed in juvenile correctional settings. Adults. The prevalence of serologic markers for current or past HBV infection among prison inmates ranges from 13% to 47%, and varies by region. Prevalence is higher among women (37%--47%) than men (13%--32%) (31,83--88) (T. Lincoln, M.D., Hampden County Correctional Center, Ludlow, Massachusetts, 2001). Chronic HBV infection is diagnosed in 1.0%--3.7% of prison inmates, 2--6 times the national prevalence estimate of 0.5% (31,83,86,88--94), and comparable to rates of chronic infection among IDUs (5%--10%) (95--98), and among MSM (1.5%--6%) (99; D. MacKellar, CDC, personal communication, 2002). Upon release, susceptible inmates are often at increased risk for infection because they resume high-risk behaviors. A study of recidivist women reported an HBV seroconversion rate of 12.2/100 person-years between incarcerations (100), compared with an estimated incidence of 0.03/100 person-years for the U.S. population (G. Armstrong, CDC, personal communication, 2002). The majority of HBV infections among incarcerated persons are acquired in the community. However, infection is also transmitted within correctional settings, and incidence rates have ranged from 0.82% to 3.8%/year (31,34,84). After identification of a single case of acute hepatitis B in a state prison, serologic testing identified acute HBV infection in 1.2% of the population (33,34). Highest rate of acute infection (8%) was determined in the dormitory of the index case and was associated with sex with another inmate. No other risk factors were associated with infection. Acute infections were also identified in other prison dormitories, and chronic HBV infection was identified in 1% of the inmate population. Serologic testing of susceptible inmates 1 year later identified an additional 3.8% who had become newly infected with HBV. Among patients with acute hepatitis B reported to CDC's Sentinel Counties Study of Viral Hepatitis, 5.6% have a history of incarceration during the disease incubation period (8). HBV transmission in the prison setting can occur through sexual activity, injection-drug use, and percutaneous exposures that are not apparent, as it does in households where persons with chronic HBV infection reside (101,102). Data are lacking regarding the prevalence of HBV infection among short- and long-term residents of jails. However, the demographic and risk factor profiles of jail and prison inmates are similar, and the burden of HBV infection and risk of transmission might be expected to be similar, especially among long-term jail residents (13,15,28,29). Correctional Staff. The overall prevalence of HBV infection was 12.6% in the only study performed among correctional workers, a rate not significantly different from that of the general population after adjusting for age and race (48). Percutaneous and mucous membrane exposures to blood were relatively infrequent, and the most frequently reported exposure was blood on the skin, which was not associated with HBV infection. Hepatitis C Virus InfectionHCV, a bloodborne pathogen, is most efficiently transmitted by direct percutaneous exposure to infectious blood. Of persons newly infected with HCV, only 20%--30% have symptoms of acute hepatitis (10,103,104). Chronic infection develops among 75%--85% of persons infected as older adults (aged >45 years) and among 50%--60% of persons infected as juveniles or young adults (105). The majority of persons with chronic HCV infection are asymptomatic, and approximately 30% have no evidence of liver disease. Among chronically infected persons, biochemical evidence of chronic liver disease develops among 70% of those infected as adults, but (on the basis of limited data) in only 10% of those infected as juveniles (105). The risk for progression to cirrhosis also varies by age at infection, from 10%--20% among persons infected as older adults to <5% among persons infected as juveniles or younger adults. In addition to age, clinical progression is also accelerated by alcohol intake, chronic coinfection with HBV, and male sex (105). Coinfection with HIV increases HCV viral loads, the rate of progression to fibrosis and cirrhosis, and liver-related mortality (106). HCC develops among 1%--5% of persons with chronic hepatitis C. Epidemiology of HCV Infection An estimated 3.9 million persons (1.8%) in the civilian, noninstitutionalized U.S. population have been infected with HCV, of whom approximately 2.7 million (1.3%) are chronically infected. In 1990, approximately two thirds of persons infected with HCV were aged 30--49 years (107). Blacks had a higher prevalence of HCV infection than whites (3.2% compared with 1.5%), and among black males aged 40--49 years, prevalence was 9.8% (107). The highest prevalence of HCV infection (70%--90%) is reported among those persons with substantial or repeated direct percutaneous exposures to blood (e.g., IDUs, persons with hemophilia treated with clotting factor concentrates that did not undergo viral inactivation, and recipients of transfusions from HCV-positive donors). Moderate infection prevalence (10%) has been reported among long-term hemodialysis patients, and lower prevalence is reported among persons with high-risk sexual practices (5%) and health-care workers (1%--2%) (10). HCV is not transmitted efficiently through occupational exposure. The risk of acquiring HCV infection from a contaminated needle stick is <2%, and transmission rarely has been documented from mucous membrane or nonintact skin exposures (47). The highest incidence of acute hepatitis C is among persons aged 20--39 years (108,109). Blacks and whites have a similar incidence of acute disease, and incidence rates are higher among males than females. Although the incidence of acute hepatitis C has declined by >80% since 1989, primarily as a result of a decrease in cases among IDUs, the major risk factor for HCV infection remains injection-drug use, which accounts for 60% of newly acquired cases (10,110,111). No association has been determined between newly acquired HCV infection and military service, medical, surgical, or dental procedures, tattooing, acupuncture, ear piercing, or foreign travel (43,44). If transmissions from such exposures do occur, the frequency has been too low to detect. Although the number of cases of acute hepatitis C among IDUs has declined dramatically since 1989, both the incidence and prevalence of HCV infection remain high among this group (98,112,113). Among IDUs, HCV is transmitted through the transfer of infected blood by sharing syringes, needles, or other drug paraphernalia contaminated with the blood of an infected person (114--116). HCV infection is acquired more rapidly after the initiation of injection-drug use than either HBV or HIV infection, and the rate of HCV infection among juvenile IDUs is four times greater than the rate of HIV infection. In 1980s studies, approximately 80% of newly initiated IDUs were infected with HCV within 2 years (98,117,118). This rapid acquisition of HCV infection was probably caused by the high prevalence of chronic HCV infection among IDUs, resulting in a greater likelihood of exposure to an HCV-infected person through sharing of drug paraphernalia. More recent studies report the rate of HCV acquisition has slowed, and only one third of IDUs are infected within 2 years after initiating injection-drug use. Nonetheless, incidence remains high at 10%--15%/year (112,116,119,120). HCV Infection in Correctional Settings Juveniles. The prevalence of HCV antibody among detained or incarcerated juveniles is estimated at 2%--3.5%. A history of injection-drug use is the predominant risk behavior, and regardless of reported risk behaviors, the prevalence is higher among females than among males (3%--7% versus 2%--3%) (A. Thomas, M.D., Oregon Health Division; and R. Bair, M.D., Bexar County Juvenile Detention Center, San Antonio, Texas; personal communications, 2001). The extent to which HCV infection is transmitted within juvenile correctional institutions is not known. Adults. Among prison inmates, 16%--41% have serologic evidence of HCV infection, and 12%--35% have chronic HCV infection; rates vary by geographic region (88,107,121,122; L. Wang, Ph.D., New York State Department of Health; D. Lau, M.D., University of Texas Medical Branch---Galveston; personal communications, 2001). HCV infection is primarily associated with a history of injection-drug use. In a Wisconsin study of 1,148 inmates, among the 310 (27%) with a history of injection-drug use and serologic evidence of HBV infection or biochemical evidence of liver disease, 91% were determined to be anti-HCV--positive (J. Pfister, M.S., Wisconsin State Laboratory of Hygiene, personal communication, 2001). Among HCV-positive entering jail inmates in Massachusetts, 85% reported needle-sharing, prior drug use, or a history of hepatitis (T. Lincoln, M.D., Hampden County Correctional Center, Ludlow, Massachusetts, personal communication, 2001). The risk of HCV acquisition during incarceration is not well-established. The only published study to examine the incidence of HCV infection among prison inmates reported a rate of 1.1 infections/100 person-years of incarceration among males (121). Correctional Staff. No published studies have reported the prevalence of HCV infection among correctional staff. In one unpublished study, among correctional health-care workers the prevalence of HCV infection was 2% (R. Gershon, Dr.P.H., Columbia University, New York, personal communication, 2002) --- no higher than in the general population. This finding is similar to that of studies among other occupational groups, including hospital-based health-care workers, surgeons, and public safety workers (10,123). Preventing and Controlling Viral HepatitisPrimary prevention of infection with hepatitis viruses can be achieved either through immunization (i.e., HAV or HBV) or through behavioral interventions to reduce risk factors for infection (i.e., HCV). In addition, identification of persons with chronic HBV and HCV infection provides an opportunity to initiate activities (e.g., counseling, treatment, or vaccination) that can prevent further disease transmission and reduce the progression of chronic liver disease. This section summarizes current information and practices to prevent infection with hepatitis viruses, including immunization, antiviral treatment, and risk-reduction counseling. Prevention of HAV InfectionStrategy To Prevent HAV Infection Preexposure Immunization. Vaccination is the most effective means to prevent HAV infection and reduce disease incidence. In the United States, preexposure vaccination is recommended for persons at highest risk for infection and persons for whom infection would result in adverse consequences (Box 1). In addition, routine vaccination is recommended for persons aged 2--19 years living in states and communities with the highest historic rates of disease (11) because conditions that contribute to communitywide transmission continue to exist. Postexposure Prophylaxis. Passive immunization with immune globulin IG is >85% effective in preventing hepatitis A after exposure of an unvaccinated person to an infected person, if administered <2 weeks after exposure (11). Anti-HAV testing is not recommended because it would delay IG administration and is likely not cost-effective. Although limited data indicate hepatitis A vaccine might provide protection when administered soon after exposure, this has not been evaluated in controlled clinical trials, and use of hepatitis A vaccine alone is not recommended for postexposure prophylaxis. However, persons who receive IG postexposure prophylaxis, and for whom hepatitis A vaccine is also recommended, require vaccination (11). Detection and Management of Acute HAV Infection The diagnosis of hepatitis A is based on a positive serologic test for IgM anti-HAV in a person with clinical signs or symptoms of acute viral hepatitis. Serologic confirmation of HAV infection is required because hepatitis A cannot be distinguished from other forms of viral hepatitis on the basis of clinical presentation alone (Box 2). Although management of clinical illness is supportive, progression to acute liver failure can occur (especially in persons with chronic liver disease), and 10%--15% of patients have relapsing illness. Contact Tracing. Cases of acute hepatitis A are reported to the appropriate public health authorities, and a contact investigation is initiated by correctional officials to identify persons who would benefit from postexposure prophylaxis. Cellmates, sexual contacts, and persons having ongoing close personal contact with the index case are administered IG (Box 3) (11). Current Practices: Prevention of HAV in Correctional Settings Nationally, the extent to which juvenile correctional systems vaccinate against hepatitis A is unknown. A recent assessment determined that in six of the 17 states where routine childhood vaccination is recommended, vaccination was also being conducted in juvenile detention facilities (CDC, unpublished data, 2002). A limited number of adult correctional systems routinely offer hepatitis A vaccination to all persons at risk for infection, whereas others offer vaccination only to inmates infected with HCV. Prevention of HBV InfectionStrategy To Prevent HBV Infection Prevention of acute and chronic HBV infection and elimination of HBV transmission in all age groups is most effectively achieved through hepatitis B vaccination (9). The national strategy to eliminate HBV transmission has four components: 1) prevention of perinatal HBV infection through maternal screening and postexposure prophylaxis of newborns of HBsAg-positive mothers; 2) hepatitis B vaccination of all infants to prevent infection in childhood and at later ages; 3) vaccination of all adolescents not previously vaccinated to prevent infection in this age group and at later ages; and 4) vaccination of adults and adolescents in groups at increased risk for infection (Box 4) (9,124). Hepatitis B vaccination has been included in routine health-care visits for adolescents, but not for adults at risk for infection (9,125). Although the majority of persons aged <19 years not covered by private insurance are covered under the Vaccines for Children Program,* similar coverage does not exist for adults, and cost reimbursement is a substantial barrier to vaccination of adults (126). Approximately 56% of persons with hepatitis B have either been treated for an STD (36%) or incarcerated (29%), factors for which routine hepatitis B vaccination is recommended (8,127). Identification of persons with chronic HBV infection through diagnostic testing can reduce risks for chronic liver disease and further transmission of infection; appropriate medical management and antiviral therapy can reduce risks for cirrhosis and HCC. Additional morbidity from other hepatic insults can be reduced through hepatitis A vaccination, alcohol-reduction counseling, and risk-reduction education. The high rate of HBV infection during sex and close contact (including with cellmates) can be prevented through vaccination. Prevention of Perinatal HBV Infection. Perinatal HBV infections can be prevented through routine testing to identify pregnant women who test positive for HBsAg and through timely postexposure immunization (prophylaxis) of their infants (78,128,129). Independent of maternal HBsAg status, hepatitis B vaccination is recommended for all infants soon after birth and before their release from the hospital (130). Initiating hepatitis B vaccination soon after birth serves as a safety net to prevent HBV infection in infants whose mothers were not tested (131). Adolescent Vaccination. Universal vaccination of infants against hepatitis B was first recommended in the United States in 1991 (9) and catch-up vaccination of all adolescents was recommended in 1995 to achieve elimination of HBV transmission in a more timely manner (132--135). Hepatitis B vaccination is now required by 33 states for entry to middle school or seventh grade. Three states have laws that require vaccination for college entry, and certain colleges require hepatitis B vaccination for matriculation (136; S. Ainsworth, American College Health Association, personal communication, 2002). Juvenile correctional vaccination programs have been established to prevent infections among detained persons at high risk for infection who might not be reached by school requirements. Completion of the vaccination series in these programs has been complicated by population turnover and the need for parental consent in certain jurisdictions. However, recidivism can bring opportunities to offer inmates second and third vaccine doses (137; G. Shostak, M.P.H., Massachusetts Department of Youth Services, personal communication, 2001). Adult Vaccination. Routine vaccination of infants, young children and adolescents is expected to eventually eliminate transmission of HBV among adults in the United States. However, decades will pass before vaccinated children become protected adults, and vaccination of adults at increased risk for infection remains essential to reducing their high incidence of disease. Vaccination coverage among adults at occupational risk for HBV infection has successfully reduced infection incidence by >90% (138). This was achieved by requiring employers to provide education and hepatitis B vaccination at no cost to employees (139). However, early efforts to vaccinate other adults had limited success, primarily because of a lack of sustained programs and coverage for vaccine cost. More recently, demonstration programs funded by state and local health departments to deliver hepatitis B vaccine in correctional facilities, and STD and substance-abuse--treatment centers, have demonstrated high vaccination coverage can be achieved (140,141). Previously, a major barrier to vaccination of adults at high risk was the practice of offering vaccine only to persons likely to complete the series. Although administration of the complete vaccine series should be the goal of any immunization program, high first-dose and modest second-dose vaccination coverage rates have been achieved when vaccine is offered to all persons in settings that serve populations at high risk (140). Protective levels of antibody develop after 1 dose of hepatitis B vaccine among 30%--50% and after 2 doses of vaccine among 75% of healthy young adults (142--144). The transient nature of adult populations in correctional facilities often prevents completion of the full hepatitis B vaccine series. Ensuring follow-up with subsequent doses requires that an immunization record is included in the medical record of all inmates, is transferred among correctional facilities, and is provided to the inmate as part of release planning. Testing for HBV Infection Pregnant Women. HBsAg testing is recommended for all pregnant women as soon as the pregnancy is recognized, irrespective of hepatitis B vaccination history or previous test results (9,145--147). In addition, women with risk factors for HBV infection during their pregnancy (e.g., intercurrent STDs, multiple sex partners, sex partners and household contacts of HBsAg-positive persons, or clinically apparent hepatitis) need retesting for HBsAg late in pregnancy because of the high risk for HBV infection (9,147). Women diagnosed with chronic infection need evaluation for chronic liver disease, and close contacts (e.g., sex, household, prison cell, or dormitory) require vaccination because of their high risk for infection (9). Prevaccination Testing. Proof of previous hepatitis B vaccination through an immunization registry, medical records, or vaccination card can be used to determine whether to exclude inmates from vaccination. When inmate vaccination status is unknown, testing for immunity to HBV infection can reduce vaccine cost among populations with high rates for infection or vaccination coverage (Box 5). However, vaccination of a person immune to HBV infection because of prior vaccination or infection does not increase risk for adverse events. Testing is not indicated before vaccination of adolescents or younger children because of the low prevalence of HBV infection in these age groups (9,148). As hepatitis B vaccination coverage increases among adolescents, a higher proportion of adults will be immune to HBV infection. Correctional systems should be aware of state hepatitis B vaccination requirements for middle school entry, which typically achieve high vaccination coverage. If adequate immunization records are not routinely available for incoming inmates, periodic serologic surveys are necessary to determine the prevalence of immunity to HBV infection and to guide policies for prevaccination testing. Among populations with a high prevalence of immunity as a result of vaccination, testing for chronic HBV infection is not warranted. However, among populations with a high prevalence of HBV infection, testing is necessary to identify inmates with chronic HBV infection and initiate medical follow-up and immunization of close contacts. Postvaccination Testing. Testing to determine antibody response to vaccination is not necessary for healthy juveniles and adults (Appendix A). For immunocompromised persons (e.g., hemodialysis patients or HIV-infected) and persons with continued known exposure to HBV infection (e.g., infants born to HBsAg-positive mothers, sex partners of HBsAg-positive persons, or health-care workers), testing is needed to verify response to vaccination and the need for possible revaccination, or to identify HBV infection (9,149,150) Prevention of HBV Infection After Exposure Immunization (active, passive, passive-active) within a relatively short period of time after exposure to HBV can effectively prevent acute and chronic infection. Initiation of the hepatitis B vaccine series within 12--24 hours of exposure has been demonstrated 70%--90% effective in preventing HBV infection (131,151). The combination of vaccine and HBIG achieves a similar level of efficacy (Box 6) (128,129). Among known nonresponders to vaccination, 1 dose of HBIG is 70%--90% effective in preventing hepatitis B when administered within 7 days of a percutaneous HBV exposure. HBIG administered within 2 weeks is also required for protection from sexual exposure to a person with acute hepatitis B (152--154). Detection of HBV Infection Acute HBV Infection. Acute HBV infection is asymptomatic among 60%--70% of patients, but can have symptoms and signs associated with acute viral hepatitis (e.g., loss of appetite, nausea, vomiting, fever, abdominal pain, or jaundice), and must be confirmed by serologic testing (Table 2, Box 2). Treatment for acute hepatitis B is supportive, consisting of rest, hydration, and symptomatic relief as needed. Identification of an inmate with acute HBV infection, especially one who has been incarcerated >6 months, requires an epidemiologic investigation by correctional officials, in collaboration with the appropriate health authorities, to identify the source of infection. Depending upon the results, vaccination of sexual, prison cell, dormitory, and household (e.g., conjugal and other family members) contacts can be indicated. Chronic HBV Infection. Chronic HBV infection can be distinguished from acute infection by serologic testing (Table 2). Inmates identified with chronic HBV infection require evaluation to determine the extent of liver disease, virus replication, indications for antiviral therapy (64), and need for vaccination of contacts to prevent HBV transmission. Management of Chronic HBV Infection Initial evaluation of patients with chronic HBV infection includes biochemical tests for liver disease (e.g., alanine aminotransferase [ALT], and aspartate aminotransferase [AST]), for the extent of liver disease (e.g., serum albumin or prothrombin time), and status of HBV replication (e.g., HBeAg, antibody to HBeAg [anti-HBe], and HBV DNA). Alpha interferon, lamivudine, or adefovir dipivoxil are approved by the Food and Drug Administration (FDA) for treatment of chronic hepatitis B (64,155). Therapy can be appropriate for patients who have abnormal levels of liver enzymes, active virus replication (HBeAg-positive or high levels of HBV DNA), and a liver biopsy indicating presence of moderate disease activity and fibrosis (64). Treatment with interferon, administered by injection 3 times/week, substantially decreases HBV DNA levels and clears HBeAg among >50% of patients with ALT levels >5 times the upper limit of normal, and among 20%--35% of patients with ALT levels 2--5 times the upper limit of normal. Among patients with ALT levels <2 times the upper limit of normal, response is poor and therapy should be deferred. Long-term follow-up of treated patients indicates remission of chronic hepatitis induced by alpha interferon is of long duration (64). Patient characteristics associated with positive response to interferon therapy include low pretherapy HBV DNA levels, high pretherapy ALT levels, short duration of infection, acquisition of disease in adulthood, and histology indicative of active inflammation. Lamivudine, administered orally daily, has been as effective as interferon at clearing HBeAg. Although a majority of patients taking lamivudine demonstrate improved liver histology, development of lamivudine-resistant HBV mutants is common, especially with prolonged use, and diminishes the effectiveness of treatment. Studies of lamivudine in combination with interferon have not been demonstrated to be superior to monotherapy (64). The newest therapy to be approved is adefovir, which also is administered orally daily. Patients treated with adefovir exhibited substantial improvements in liver histology and decreased levels of HBV DNA; however, durability of the response has not been determined (156). Adefovir has been demonstrated to be effective in patients with chronic hepatitis B who have experienced resistance to lamivudine (156). Treatment of persons coinfected with HIV and HBV requires additional monitoring. After initiation of highly active antiretroviral therapy (HAART) for treatment of HIV infection, reactivation of HBV replication with development of acute hepatitis has been observed among persons thought to have resolved HBV infection. Although interferon treatment is not as effective for patients coinfected with HIV, HBV and HIV can be simultaneously treated (157). Inmates identified with chronic HBV infection can benefit from counseling regarding ways to prevent transmitting HBV infection to others. Vaccination of sexual and nonsexual contacts (e.g., cellmates) can also prevent transmission (9). Current Practices: Prevention of HBV in Correctional Settings Juveniles. Juveniles in the justice system have been determined to have increased risk for HBV infection (125). In 2001, a national survey of state juvenile correctional systems reported that 36 (86%) of 42 responding systems had a hepatitis B prevention program in place; 78% used the VFC program to pay for vaccine; and 85% considered vaccination to be a corrections responsibility while a juvenile is in custody. Written hepatitis B prevention policies were in place in 65% of states, and 27% used a vaccine tracking system or immunization registry (CDC, unpublished data, 2002). In states with immunization registries and VFC participation, vaccination coverage among incarcerated juveniles has reached levels >90% (G. Treder, Wisconsin Department of Corrections, personal communication, 2002). However, where the correctional system does not have legal guardianship of the detained juvenile, the need for parental consent can pose a barrier to vaccination. In states with laws enabling minors to consent to their own STD-related treatment and prevention, hepatitis B has been included, facilitating implementation of vaccination programs (M. Staples-Horne, M.D., Georgia Department of Juvenile Justice, personal communication, 2002). Adults. Hepatitis B vaccination is recommended for adults in correctional settings because of their increased risk for infection, both inside and outside of prisons and jails (9,33,34,100). Vaccinating inmates in prisons has been demonstrated feasible and cost-saving from both prison and outside community perspectives (158) (CDC, unpublished data, 2002). Approximately 25 state correctional systems and the Federal Bureau of Prisons have implemented hepatitis B immunization programs, which vary in scope and are often limited by funding or staffing resources. System policies include immunization of 1) all incoming inmates; 2) inmates of certain ages; 3) inmates with certain lengths of sentences; 4) inmates with HCV infection; or 5) inmates who request vaccination. In certain correctional systems, inmates must pay for vaccination (137,159). Among inmates in three systems (in Massachusetts, Michigan, and Texas) that offer hepatitis B vaccine, 60%--80% accept vaccination (T. Lincoln, M.D., Hampden County Correctional Center, Ludlow, Massachusetts; D. Thelen, Michigan State Department of Corrections; M. Hurie, Michigan State Department of Health; and M. Kelley, M.D., Texas Department of Criminal Justice; personal communications, 2001). Successful hepatitis B vaccination programs, like other successful adult vaccination programs (e.g., influenza) include establishment of policies for vaccination and a source of payment for vaccine (160--163). Among states, Hawaii, Michigan, Texas, and Wisconsin have extensive experience in offering vaccine to inmates. The Texas Department of Criminal Justice has 105 adult facilities with approximately 145,000 inmates. In 1999, funds were appropriated for hepatitis B vaccination of all offenders. A cost analysis indicated prevaccination testing would be cost-effective if prior HBV infection rates were >25%. However, a seroprevalence study identified an HBV prevalence of 17.8% and a history of vaccination among another 5.5%. Medical records are reviewed for a history of hepatitis B vaccination or evidence of HBV infection from prior clinical testing. All inmates are offered vaccine, and the central pharmacy delivers second and third doses of vaccine to the appropriate housing units on a 0-, 2-, and 4-month vaccination schedule. Scheduled vaccine doses are listed in each inmate's medical record to serve as an additional reminder to complete the vaccination series. In the first 18 months of the program, 115,627 previously incarcerated inmates initiated the vaccine series, and since November 2001, the program has vaccinated all inmates at entry --- an estimated 35,000/year. The estimated cost for vaccination of 121,000 inmates during the first 18 months of the program was $8 million, with an expected recurring annual cost of $2.6 million to vaccinate incoming inmates (M. Kelley, M.D., Texas Department of Criminal Justice, personal communication, 2001). Prevention of HCV InfectionStrategy To Prevent HCV Infection CDC's national strategy to prevent HCV infection includes 1) prevention of transmission during high-risk activities (e.g., injection-drug use and unprotected sex with multiple partners) through risk-reduction counseling, testing, and appropriate medical management of infected persons; 2) donor screening and product inactivation procedures to eliminate transmission from blood, blood products, donor organs, and tissue; and 3) improved infection control practices to further reduce risk of transmission during medical procedures † (10). Primary prevention is directed at lowering the incidence of HCV infection. Of the estimated 25,000--40,000 persons newly infected with HCV annually during the past 5 years, approximately 60% acquired their infection through injection-drug use (45,111). Because no vaccine exists to prevent HCV infection, prevention must focus on risk reduction through counseling of persons who have admitted to or are at risk for illicit drug use or high-risk sexual practices. Counseling and testing to prevent HCV infection should be conducted in settings where persons at high risk are identified, including correctional health programs, and clinics that treat STDs, HIV/AIDS, and substance abuse (10) (Box 7). The high prevalence of HCV infection and risk associated with HCV infection among inmates requires inclusion of HCV prevention activities in correctional settings. To be effective, risk reduction among this population often requires a multidisciplinary approach to address drug use as well as other medical, psychological, social, vocational, and legal problems (164). Identification of HCV-infected persons is required to initiate secondary and tertiary prevention activities to reduce the risks for HCV transmission and chronic liver disease (10). Anti-HCV--positive persons require further evaluation for chronic HCV infection and liver disease, and persons with chronic hepatitis C require evaluation for possible antiviral therapy and the need for further medical management. Persons with chronic hepatitis C are at risk for increased morbidity from additional hepatic insults. Fulminant hepatitis caused by hepatitis A can be prevented by vaccination (50). HCV-infected persons often have risk factors for HBV infection; therefore, hepatitis B vaccination is also recommended (10). Persons with hepatitis C should be counseled to not use alcohol, because its use (>10g/day for women and >20g/day for men) has been associated with more rapid progression to cirrhosis, which puts patients at higher risk for HCC (10,165,166). Persons at risk for HCV infection or those chronically infected with HCV can benefit from health education on topics including 1) substance-abuse treatment where appropriate, 2) clean needle and syringe use, 3) risks of sharing drug paraphernalia, and 4) condom use (10). Counseling and educational materials should include information concerning reducing further liver damage, as well as treatment options for those with chronic liver disease. Release planning should include substance-abuse--treatment referrals for IDUs and medical referrals to specialists for future medical management and treatment (see juvenile and adult sections on health education and release planning). Testing for HCV Infection Anti-HCV testing is recommended to identify infected persons. To prevent reporting of false-positive results, testing should include both an antibody screening assay (e.g., enzyme immunoassay [EIA]) and supplemental or confirmatory testing with an additional, more specific assay (e.g., recombinant immunoblot assay [RIBA,® Chiron Corporation, Emeryville, California] for anti-HCV or nucleic acid testing for HCV RNA). These tests detect anti-HCV in >97% of infected patients but do not distinguish between acute, chronic, or resolved infection (11). Substantial variation exists among laboratories regarding the extent to which more specific testing is performed. The level of the screening test signal-to-cut--off ratio has been demonstrated to predict a true antibody-positive result. Use of the signal-to-cut--off ratio limits supplemental testing to those samples for which the ratio is low (167). Detection of HCV Infection Acute Hepatitis C. Acute HCV infection is usually asymptomatic (80%). However, acute hepatitis C should be included in the differential diagnosis of inmates who have signs and symptoms of acute hepatitis (Box 2). Confirmation of acute hepatitis C requires negative test results for IgM anti-HAV and IgM anti-HBc and a positive screening test result for anti-HCV, verified by supplemental testing or a high signal-to-cut--off ratio. Among a limited number of patients, onset of symptoms may precede anti-HCV seroconversion, and follow-up antibody testing might be necessary to make the diagnosis. Identification of an inmate with acute hepatitis C, especially a person incarcerated for >6 months, requires initiation of an epidemiologic investigation by correctional officials, in collaboration with the appropriate health authorities, to identify the source of infection. Depending upon the results, testing of contacts might be indicated. Chronic HCV Infection. Anti-HCV alone does not distinguish between acute, chronic, or resolved infection. In persons testing positive for anti-HCV, chronic HCV infection can be distinguished by persistence of HCV RNA for >6 months. Management of HCV Infection HCV-positive persons benefit from evaluation for the presence and severity of chronic liver disease. Antiviral therapy is recommended for persons with persistently elevated ALT levels, detectable HCV RNA, and a liver biopsy that indicates either portal or bridging fibrosis or moderate degrees of inflammation and necrosis. No clear consensus exists on whether to treat patients with persistently normal serum transaminases. Information is available on the National Institute of Health (NIH) website§ regarding regimens with proven efficacy approved by the FDA for the treatment of chronic hepatitis C (168). The FDA has approved three antiviral therapies for treatment of chronic hepatitis C in persons aged >18 years: alpha interferon, pegylated interferon, and alpha or pegylated interferon in combination with ribavirin. All are administered for <52 weeks. Among persons with HCV genotype 1, the most common genotype in the United States, the response rate to either of the interferons administered alone is <20%, but the response rate to the combination of alpha interferon and ribavirin is 30%--40%, and to pegylated interferon and ribavirin, 40%--50%. Both the alpha and pegylated interferons are administered by injection; ribavirin is taken orally. All of these drug regimens have side effects, certain of which can be serious. Successful treatment eliminates viremia and the potentials for HCV transmission and further chronic liver disease (168,169). Among persons with both HCV and HIV infection, benefits of therapy for chronic hepatitis C have only recently been evaluated. The decision to treat persons coinfected with HIV must take into consideration concurrent medications and medical conditions (e.g., hyperthyroidism, renal transplant, or autoimmune disease). If CD4 counts are normal or minimally abnormal (>500/mL), treatment responses to interferon monotherapy are similar to non-HIV--infected persons (106,170,171). The efficacy of ribavirin/interferon combination therapy among HIV-infected persons has been tested in only a limited number of patients. Ribavirin can have substantial interactions with other antiretroviral drugs (168). Each patient should be evaluated by a physician familiar with the treatment of patients with HCV infection and HIV infections when appropriate, and indications for therapy should be reassessed at regular intervals. Current Practices: Prevention of HCV in Correctional Settings Testing populations with high proportions of IDUs is an efficient strategy for identifying HCV-positive persons (10). However, in the correctional setting, only a limited number of studies have examined willingness to be tested, treatment options, compliance, and outcomes among those offered therapy (122,172). In assessments of other prison screening programs (e.g., for HIV and STDs), a relatively high rate (approximately 50%) of refusal has been reported (173--175). Limited data from studies in Rhode Island and Pennsylvania indicate approximately 7%--27% of all inmates identified with HCV infection ultimately begin treatment (122,172; F. Maue, M.D., Pennsylvania State Department of Corrections, personal communication, 2001). The majority of inmates were excluded from treatment because of clinical contraindications, short lengths of prison stay, and drug or alcohol use (122,172; F. Maue, M.D., Pennsylvania State Department of Corrections, personal communication, 2001). Less-restrictive criteria might increase the number of inmates eligible for treatment (168). However, factors contributing to acceptance and completion of treatment regimens need to be identified to improve outcomes. Health EducationHealth education directed toward prevention of viral hepatitis includes information related to the disease, routes of transmission, risk factors for infection, methods of prevention, disease outcomes, and treatment options. During incarceration, numerous educational opportunities exist (e.g., at entry, or in HIV-education and other classes). Education can take different forms, including videos, brochures, and formal classroom presentations. However, repeated face-to-face sessions have been determined the most effective means with the highest retention (Box 8) (176--178). Model programs use peer health educators in workshops for incoming inmates, and community educators to discuss risk assessment, risk reduction, and referrals for soon-to-be released inmates.¶ Health education programs aimed at reducing risk of infection with hepatitis viruses include discussion of hepatitis A prevention, hygiene practices, and the significance of vaccination for persons at risk for infection. Curricula addressing HBV and HCV infections include information concerning the similar modes of transmission and means for prevention, and information about hepatitis B vaccination and risk reduction. Such information can also be incorporated into health-education programs for the prevention of HIV/AIDS. Release PlanningRelease planning is a relatively new component of health-care management for incarcerated persons. The majority of medical release and discharge planning programs in prison facilities have focused on HIV aftercare (179,180), but management of other chronic infections can result in the same beneficial outcomes. Comprehensive release planning includes transitional housing, continued access to discharge medications and immunizations, and coordination and case-management of long-term specialized care for persons with chronic conditions. Persons diagnosed with chronic HBV infection can benefit from counseling related to preventing transmission to household, sexual, and drug-use contacts. Susceptible contacts of persons diagnosed with chronic HBV infection benefit from hepatitis B vaccination. Persons with chronic hepatitis B or chronic hepatitis C can benefit from 1) counseling regarding ways to reduce further liver damage, 2) referrals to substance-abuse--treatment and other IDU programs if indicated, and 3) medical referrals to specialists for future treatment. Rationale for Prevention and Control of Viral Hepatitis in Correctional SettingsThe high prevalence of chronic HBV and HCV infections and risk factors for their transmission make prevention and control of these infections high priorities for correctional health programs. In addition, because a substantial proportion of releasees to the community continue to acquire or transmit these infections at a high rate, correctional efforts should become part of prevention and control efforts in the broader community. Highly effective and safe vaccines are available to prevent HAV and HBV infections. Identification of risk factors and infection status, combined with harm- and risk-reduction counseling, and substance-abuse treatment, have the potential to prevent HCV infections in the same manner they have reduced the risk of HIV/AIDS. In addition, identification of persons with chronic HBV and HCV infection provides opportunities for medical evaluation and treatment of chronic liver disease, and measures to prevent further transmission. The feasibility of including viral hepatitis prevention activities in existing prevention programs has been demonstrated. However, the challenges to integration of a comprehensive viral hepatitis prevention and control program in correctional health settings are substantial. They include budgetary and staffing constraints, priorities that compete with preventive health care, and lack of communication among correctional health, public health, and private health-care systems. The recommendations for prevention and control of viral hepatitis that follow are adapted to the correctional setting. The objective of these recommendations is to reduce transmission of hepatitis virus infections both during and after incarceration. Implementation of these recommendations can 1) reduce transmission of HAV infection in the community by immunizing incarcerated persons at highest risk for infection; 2) eliminate transmission of HBV infection among the inmate population through immunization; 3) reduce the number of new HCV infections by testing, harm- and risk-reduction counseling, and substance-abuse treatment and prevention; 4) reduce the burden of viral hepatitis-related chronic liver disease through appropriate medical management; and 5) prevent HBV and HCV infections among correctional employees. Rating the RecommendationsThe following recommendations are rated, where applicable, on the basis of the strength of evidence indicating changes in outcomes attributable to the interventions. Where formal recommendations previously have been published, they are cited as supporting evidence and can be referred to for the original studies. Ratings have been assigned by using a modification of criteria published by the Guide to Community Preventive Services (181). No rating was assigned to a recommendation considered standard practice (i.e., a medical or administrative practice conducted routinely by qualified persons experienced in their fields).
|