Incorporating HIV Prevention into the Medical Care of
Persons Living with HIV
Recommendations of CDC, the Health Resources and
Services Administration, the National Institutes of Health, and the HIV
Medicine Association of the Infectious Diseases Society of America
Please note:
An erratum has been published for this article. To view the
erratum, please click here and
an update has been published for this report. To view the update, please click here.
The material in this report originated in the National
Center for HIV, STD and TB Prevention, Harold W. Jaffe, M.D., Director;
Division of HIV/AIDS Prevention � Surveillance and Epidemiology, Robert S.
Janssen, Director; Division of HIV/AIDS Prevention � Intervention,
Research, and Support, Robert S. Janssen, M.D., Acting Director.
Summary
Reducing transmission of human immunodeficiency virus (HIV) in the United States requires new strategies,
including emphasis on prevention of transmission by HIV-infected persons. Through ongoing attention to prevention, risky sexual and needle-sharing behaviors among persons with HIV infection can be reduced and transmission of HIV infection
prevented. Medical care providers can substantially affect HIV transmission by screening their HIV-infected patients for risk behaviors; communicating prevention messages; discussing sexual and drug-use behavior; positively reinforcing changes to safer
behavior; referring patients for services such as substance abuse treatment; facilitating partner notification, counseling, and testing; and identifying and treating other sexually transmitted diseases (STDs).
To help incorporate HIV prevention into the medical care of HIV-infected persons, CDC, the Health Resources and
Services Administration, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society
of America developed these recommendations. The recommendations are general and apply to incorporating HIV prevention
into the medical care of all HIV-infected adolescents and adults, regardless of age, sex, or race/ethnicity. They are intended for
all persons who provide medical care to HIV-infected persons (e.g., physicians, nurse practitioners, nurses, physician assistants); they might also be useful to those who deliver prevention messages (e.g., case managers, social workers, health educators).
The recommendations were developed by using an evidence-based approach. For each recommendation, the strength of
the recommendation, the quality of available evidence supporting the recommendation, and the outcome for which
the recommendation is rated are provided. The recommendations are categorized into three major components: screening for HIV transmission risk behaviors and STDs, providing brief behavioral risk-reduction interventions in the office setting and
referring selected patients for additional prevention interventions and other related services, and facilitating notification and counseling of sex and needle-sharing partners of infected persons.
Introduction
Despite substantial advances in the treatment of human
immunodeficiency virus (HIV) infection, the estimated number
of annual new HIV infections in the United States has remained at 40,000 for over 10 years
(1). HIV prevention in this country has largely focused on persons who are not HIV infected, to help them avoid becoming infected. However, further reduction of HIV transmission will require new strategies, including increased emphasis on preventing transmission by
HIV-infected persons (2,3). HIV-infected persons who are aware of their HIV infection tend to reduce behaviors that might transmit HIV
to others (4--7). Nonetheless, recent reports
suggest that such behavioral changes often are not maintained and that a
substantial number of HIV-infected persons continue to engage in behaviors that place others at risk for HIV infection
(8--13).
Reversion to risky sexual behavior might be as important in HIV transmission as failure to adopt safer sexual
behavior immediately after receiving a diagnosis of HIV
(14). Unprotected anal sex appears to be occurring more frequently in
some urban centers, particularly among young men who have sex with men (MSM)
(15). Bacterial and viral sexually
transmitted diseases (STDs) in HIV-infected men and women receiving outpatient care have been increasingly noted
(16,17), indicating ongoing risky behaviors and opportunities for HIV transmission. Further, despite declining syphilis prevalence in the
general U.S. population, sustained outbreaks of syphilis among MSM, many of whom are HIV infected, continue to occur in
some areas; rates of gonorrhea and chlamydial infection have also risen for this population
(18--21). Rising STD rates among MSM indicate increased potential for HIV transmission, both because these rates suggest ongoing risky behavior and because STDs have a synergistic effect on HIV infectivity and susceptibility
(22). Studies suggest that optimism about the effectiveness
of
highly active antiretroviral therapy (HAART) for HIV may be contributing to relaxed attitudes toward safer sex practices and increased sexual risk-taking by some HIV-infected persons
(12,23--27).
Injection drug use also continues to play a key role in the HIV epidemic; at least 28% of AIDS cases among adults
and adolescents with known HIV risk category reported to CDC in 2000 were associated with injection drug use
(28). In some large drug-using communities, HIV seroincidence and seroprevalence among injection drug users (IDUs) have
declined in recent years (29,30). This decline has been attributed to several factors, including increased use of sterile injection equipment, declines in needle-sharing, shifts from injection to noninjection methods of using drugs, and cessation of drug use (31--33). However, injection-drug use among young adult heroin users has increased substantially in some areas
(34,35), a reminder that, as with sexual behaviors, changes to less risky behaviors may be
difficult to sustain.
Clinicians providing medical care to HIV-infected persons can play a key role in helping their patients reduce risk
behaviors and maintain safer practices and can do so with a feasible level of effort, even in constrained practice settings. Clinicians can greatly affect patients' risks for transmission of HIV to others by performing a brief screening for HIV transmission
risk behaviors; communicating prevention messages; discussing sexual and drug-use behavior; positively reinforcing changes to safer behavior; referring patients for such services as substance abuse treatment; facilitating partner notification, counseling, and testing; and identifying and treating other STDs
(36,37). These measures may also decrease patients' risks of acquiring
other STDs and bloodborne infections (e.g., viral hepatitis). Managed care plans can play an important role in HIV prevention
by incorporating these recommendations into their practice guidelines, educating their providers and enrollees, and
providing condoms and educational materials. In the context of care, prevention services might be delivered in clinic or
office environments or through referral to community-based programs. Some clinicians have expressed concern that reimbursement is often not provided for prevention services and note that improving reimbursement for such services might enhance
the adoption and implementation of these guidelines.
This report provides general recommendations for incorporating HIV prevention into the medical care of all
HIV-infected adolescents and adults, regardless of age, sex, or race/ethnicity. The recommendations are intended for all persons who provide medical care to HIV-infected persons (e.g., physicians, nurse practitioners, nurses, physician assistants). They may also be useful to those who deliver prevention messages (e.g., case managers, social workers, health educators).
Special considerations may be needed for some subgroups (e.g., adolescents, for whom laws and regulations might exist
governing providing of services to minors, the need to obtain parental consent, or duty to inform). However, it is beyond the scope of this report to address special considerations of subgroups. Furthermore, the recommendations focus on sexual and
drug-injection behaviors, since these behaviors are responsible for nearly all HIV transmission in the United States. Separate guidelines have been published for preventing perinatal transmission
(38--40).
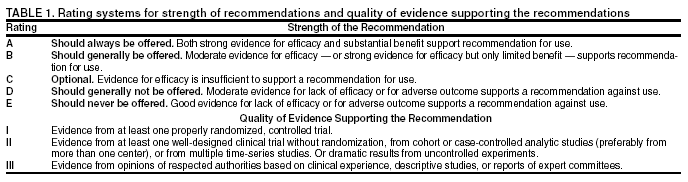
These recommendations were developed by using an
evidence-based approach (Table 1). The strength of
each recommendation is indicated on a scale of A (strongest recommendation for) to E (recommendation against); the quality of available evidence supporting the recommendation is indicated on a scale of I (strongest evidence for) to III (weakest evidence for), and the outcome for which the recommendation is rated is provided. The recommendations are categorized into three major components: 1) screening for HIV transmission risk behaviors and STDs, 2) providing brief
behavioral risk-reduction interventions in the office setting and referring
selected patients for additional prevention interventions and
other related services, and 3) facilitating notification and counseling of sex and needle-sharing partners of infected persons.
This report was developed by CDC, the Health Resources and Services Administration (HRSA), the National Institutes
of Health (NIH), and the HIV Medicine Association (HIVMA) of the Infectious Diseases Society of America (IDSA).
The recommendations will evolve as results from ongoing
behavioral intervention trials become available.
Risk Screening
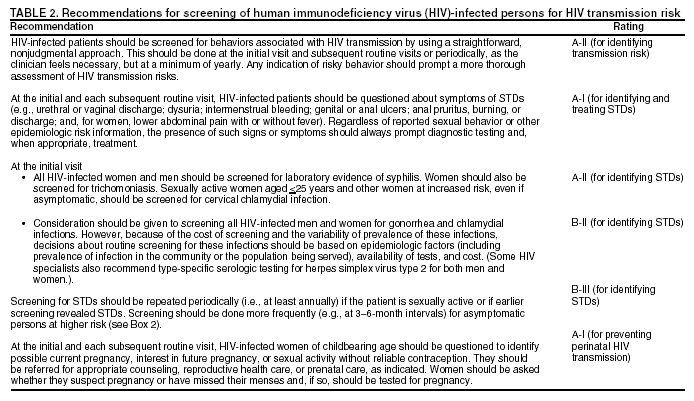
Risk screening is a brief assessment of behavioral and clinical factors associated with transmission of HIV and other STDs (Table 2). Risk screening can be used to identify patients who should receive more in-depth risk assessment and HIV
risk-reduction counseling, other risk-reduction interventions, or referral for other services (e.g., substance abuse treatment). Risk screening identifies patients at greatest risk for transmitting HIV so that prevention and referral recommendations can
be focused on these patients. Screening methods include probing for behaviors associated with transmission of HIV and other STDs, eliciting patient reports of symptoms of other STDs, and laboratory testing for other STDs. Although each of these
methods has limitations, a combination of methods should increase the sensitivity and effectiveness of screening. In
conducting risk screening, clinicians should recognize that risk is not static. Patients' lives and circumstances change, and a patient's risk
of transmitting HIV may change from one medical encounter to another. Also, clinicians should recognize that working
with adolescents may require special approaches and should be aware of and adhere to all laws and regulations
related to providing services to minors.
Screening for Behavioral Risk Factors
Clinicians frequently believe that patients are uncomfortable disclosing personal risks and hesitant to respond to
questions about sensitive issues, such as sexual behaviors and illicit drug use. However, available evidence suggests that patients, when asked, will often disclose their risks
(41,42) and that some patients have reported greater confidence in their clinician's ability
to provide high-quality care if asked about sexual and STD history during the initial visits
(43).
Screening for behavioral risk factors can be done with brief self-administered written questionnaires; computer-, audio-, and video-assisted questionnaires; structured face-to-face
interviews; and personalized discussions
(41,44--53). Screening questions can be either open-ended or closed (directed)
(Box 1). Use of open-ended questions avoids simple "yes" or "no"
responses and encourages patients to discuss personal risks and the circumstances in which risks occur (15,44,54). Open-ended questions also help the clinician gather enough detail to
understand potential transmission risks and make more
meaningful recommendations. However, although well
received by patients, the open-ended approach may initially be difficult
for clinicians schooled in directed questioning, who tend to prefer directed screening questions. Directed questions are
probably useful for identifying patients with problems that should be more thoroughly discussed. Among directed
approaches, technical tools like computer-, audio-, and video-assisted interviews have been found to elicit more self-reported risk behaviors than did interviewer-administered questionnaires, particularly among younger patients
(41,51--53,55). Studies suggest that
clinicians who receive some training, particularly that including role-play and feedback concerning clinical performance, are more
likely to perform effective risk screening
(46--49).
Sex-related behaviors important to address in risk screening include whether the patient has been engaging in sex;
number and sex of partners; partners' HIV serostatus (infected, not infected, or unknown); types of sexual activity (oral, vaginal, or
anal sex) and whether condoms are used; and barriers to abstinence or correct condom use (e.g., difficulty talking with
partners about or disclosing HIV serostatus, alcohol and other drug use before or during sex). Also, because the risk for perinatal
HIV transmission is high without appropriate intervention, clinicians are advised to assess whether women of childbearing age might be pregnant, are interested in becoming pregnant, or are not specifically considering pregnancy but are sexually active and not using reliable contraception (39,56,57). Women who are unable to become pregnant
because of elective sterilization, hysterectomy, salpingo-oophorectomy, or other medical reasons might be less likely to use condoms because of a lack of concern for contraception; these women should be counseled regarding the need for use of condoms to prevent transmission
of HIV. Patients who wish to conceive and whose partner is not infected also might
engage in risky behavior. Patients interested in pregnancy, for themselves or their partner, should be referred to a reproductive health specialist (58).
Injection-drug--related behaviors important to address in screening include whether the patient has been injecting
illicit drugs; whether the patient has been sharing needles and
syringes or other injection equipment; how many partners the
patient has shared needles with; whether needle-sharing partners are known to be HIV infected, not infected, or of
unknown HIV serostatus; whether the patient has been using new or sterilized needles and syringes; and what barriers exist to ceasing illicit drug use or, failing that, to adopting safer injection practices (e.g., lack of access to sterile needles and syringes).
Approaches to Screening for Behavioral Risk Factors
The most effective manner for screening for behavioral risk factors is not well defined; however, simple approaches are
more acceptable to both patients and health-care providers
(53). Screening tools should be designed to be as sensitive as possible
for identifying behavioral risks; a more detailed, personalized assessment can then be used to improve specificity and
provide additional detail. The sensitivity of screening instruments depends on obtaining accurate information. However, accuracy of information can be influenced by a variety of factors: recall, misunderstanding about risk, legal concerns, concern
about confidentiality of the information and how the information will be used, concern that answers may affect ability to receive services, concern that answers may affect social desirability (i.e., the tendency to provide responses that will avoid criticism), and the desire for social approval (the tendency to seek praise)
(45,55). Interviewer factors also influence the accuracy
of
information. Surveys indicate that patients are more likely to discuss risk behaviors if they perceive their clinicians
are comfortable talking about stigmatized topics such as sex and drug use
(46--49) and are nonjudgmental, empathetic, knowledgeable, and comfortable counseling patients about sexual risk factors
(41,46--50). These factors need to be
considered when interpreting responses to screening questions. To the extent possible, screening and interventions should be individualized to meet patient needs. Examples of two screening approaches are provided (Box 1).
Incorporating Screening for Behavioral Risk Factors into the Office Visit
Before the patient is seen by the clinician, screening for
behavioral risks can be done with a self-administered questionnaire;
a computer-, audio-, or video-assisted questionnaire; or a brief interview with ancillary staff; the clinician can then review
the results on the patient's medical record. Alternatively, behavioral risk screening can be done during the medical
encounter (e.g., as part of the history); either open-ended questions or a checklist approach with in-depth discussion about positive responses can be used (Box 1). Because, given patients' immediate health needs, it can be difficult in the clinical care setting to remember less urgent matters such as risk screening and harm reduction, provider reminder systems (e.g., computerized reminders)
have been used by health-care systems to help ensure that recommended procedures are done regularly. Multicomponent
health-care system interventions that include a provider reminder system and a provider education program are effective in increasing delivery of certain prevention services
(59). Risk screening might be more likely to occur in managed care settings if
the managed care organization specifically calls for it
(60).
Screening for Clinical Risk Factors
Screening for STDs
Recommendations for preventive measures, including medical screening and vaccinations, that should be included in the
care of HIV-infected persons
(16,21,39,44,54,61--69) have been published previously. This report is not intended
to duplicate existing recommendations; it addresses screening specifically to identify clinical factors associated with increased risk for transmission of HIV from infected to noninfected persons. In this context, STDs are the primary infections of concern for three reasons. First, the presence of STDs often suggests recent or ongoing sexual behaviors that may result in
HIV transmission. Second, many STDs enhance the risk for HIV transmission or acquisition
(22,70--73). Early detection and treatment of bacterial STDs might reduce the risk for HIV transmission. Third, identification and treatment of STDs can reduce the potential for spread of these infections among high-risk groups (i.e., sex or drug-using networks).
Screening and diagnostic testing serve distinctly different purposes. By definition, screening means testing on the basis of
risk estimation, regardless of clinical indications for testing, and is a cornerstone of identifying persons at risk for transmitting
HIV to others. Clinicians should routinely ask about STD symptoms, including urethral or vaginal discharge;
dysuria; intermenstrual bleeding; genital or anal ulcers or other lesions; anal pain, pruritus, burning, discharge, or bleeding; and,
for women, lower abdominal pain with or without fever. Regardless of reported sexual behavior or other epidemiologic
risk information, the presence of such symptoms should always prompt diagnostic testing and, when appropriate,
treatment. However, clinical symptoms are not sensitive for identifying many infections because most STDs are asymptomatic
(74--81); therefore, laboratory screening of HIV-infected
persons is an essential tool for identifying persons at risk for transmitting
HIV and other STDs.
Laboratory Testing for STDs
Identification of syphilis requires direct bacteriologic (i.e., dark-field microscopy) or serologic testing. However,
noninvasive, urine-based nucleic acid amplification tests (NAATs) have greatly simplified testing for
Neisseria gonorrhoeae and Chlamydia
trachomatis. Although they are more costly than other screening tests, their ease of use and sensitivity---similar to the
sensitivity of culture for detection of N.
gonorrhoeae and substantially higher than the sensitivity of all other tests for
C. trachomatis (including culture)---for detecting genital
infection are great advantages. Detection of rectal or pharyngeal gonorrhea
still requires culture. Pharyngeal infection with
C. trachomatis is uncommon, and routine screening for it is not
recommended (63,82). NAATs have not been approved for use with specimens collected from sites other than the urethra, cervix, or
urine. Recommended screening strategies and diagnostic tests for detecting asymptomatic STDs are described (Box 2,
Table3).
Local and state health departments have reporting requirements, which vary among states, for HIV and other
STDs. Clinicians need to be aware of and comply with requirements for the areas in which they practice; information on
reporting requirements can be obtained from health departments.
Screening for Pregnancy
Women of childbearing age should be questioned during routine visits about the possibility of pregnancy. Women who state that they suspect pregnancy or have missed their menses should be tested for pregnancy. Early pregnancy diagnosis
would benefit even women not receiving antiretroviral treatment because they could be offered treatment to decrease the risk for perinatal HIV transmission.
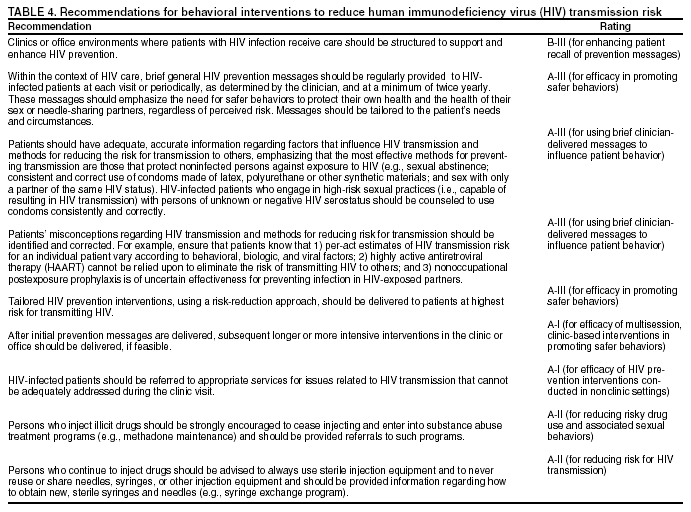
Behavioral Interventions
Behavioral interventions are strategies designed to change persons' knowledge, attitudes, behaviors, or practices in order to reduce their personal health risks or their risk of
transmitting HIV to others (Table 4). Behavioral change can be facilitated
by environmental cues in the clinic or office setting, messages delivered to patients by clinicians or other qualified staff on-site, or referral to other persons or organizations providing prevention services. Because behavior change often occurs in
incremental steps, a brief behavioral intervention
conducted at each clinic visit could result in patients, over time, adopting and
maintaining safer practices. Behavioral interventions
should be appropriate for the patient's culture, language, sex, sexual orientation,
age, and developmental level (44). In settings where care is delivered to HIV-infected adolescents, for example, approaches need to be specifically tailored for this age group
(83). Also, clinicians should be aware of and adhere to all laws and regulations
related to providing services to minors.
Structural Approaches To Support and Enhance Prevention
Clinic or office environments can be structured to support and enhance prevention. All patients, especially new
patients, should be provided printed information about HIV transmission risks, preventing transmission of HIV to others, and preventing acquisition of other STDs. Information can be disseminated at various locations in the clinic; for example, posters and other visual cues containing prevention messages can be displayed in examination rooms and waiting rooms. These materials usually can be obtained through local or state health department HIV/AIDS and STD programs or from
the National Prevention Information Network (NPIN) (1-800-458-5231;
http://www.cdcnpin.org). Additionally, condoms
should be readily accessible at the clinic. Repeating prevention messages throughout the patient's clinic visit reinforces their importance, increasing the likelihood that they will be remembered
(68).
Interventions Delivered On-Site
Prevention Messages for All Patients
All HIV-infected patients can benefit from brief prevention messages emphasizing the need for safer behaviors to protect both their own health and the health of their sex or needle-sharing partners. These messages can be delivered by
clinicians, nurses, social workers, case managers, or health educators. They include discussion of the patient's responsibility for appropriate disclosure of HIV serostatus to sex and needle-sharing partners. Brief clinician-delivered approaches have
been effective with a variety of health issues, including depression
(84), smoking (85--90), alcohol abuse
(91,92), weight and diet (93), and physical inactivity
(94). This diverse experience with other health behaviors suggests that similar approaches may
be effective in reducing HIV-infected patients' transmission risk behaviors. For patients already taking steps to reduce their risk of transmitting HIV, hearing the messages can reinforce continued risk-reduction behaviors. These patients should
be commended and encouraged to continue these behaviors.
General HIV Prevention Messages
Patients frequently have inadequate information regarding factors that influence HIV transmission and methods
for preventing transmission. The clinician should ensure that patients understand that the most effective methods for
preventing HIV transmission remain those that protect noninfected persons against exposure to HIV. For sexual transmission, the only
certain means for HIV-infected persons to prevent sexual transmission to noninfected persons are sexual abstinence or sex
with only a partner known to be already infected with HIV. However, restricting sex to partners of the same serostatus does
not protect against transmission of other STDs or the possibility of HIV superinfection unless condoms of latex, polyurethane, or other synthetic materials are consistently and correctly used. Superinfection with HIV has been reported and appears to be rare, but its clinical consequences are not known
(95,96). For injection-related transmission, the only certain means for
HIV-infected persons to prevent transmission to noninfected persons are abstaining from injection drug use or, for IDUs who are unable or unwilling to stop injecting drugs, refraining from sharing injection equipment (e.g.,
syringes, needles, cookers, cottons, water) with other persons. Neither antiretroviral therapy for HIV-infected persons nor postexposure prophylaxis for partners is a reliable substitute for adopting and maintaining behaviors that guard against HIV exposure
(97).
Identifying and Correcting Misconceptions
Patients might have misconceptions about HIV transmission
(98), particularly with regard to the risk for HIV
transmission associated with specific behaviors, the effect of antiretroviral therapy on HIV transmission, or the effectiveness of postexposure prophylaxis for nonoccupational exposure
to HIV.
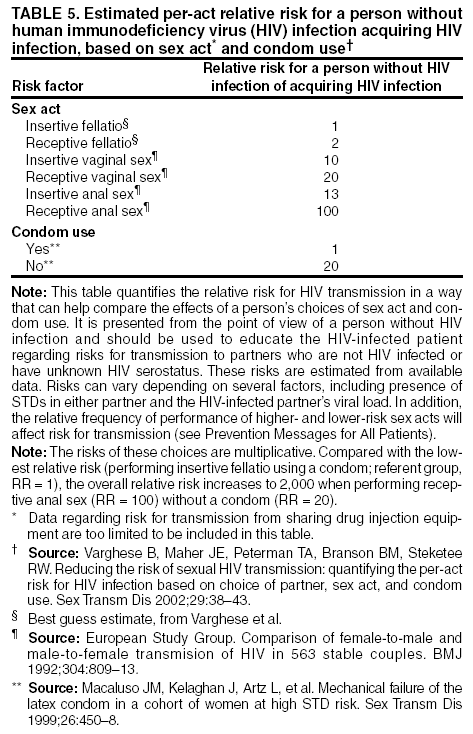
Risk for HIV Transmission Associated with Specific Sexual
Behaviors. Patients often ask their clinicians about the
degree of HIV transmission risk associated with specific sexual activities. Numerous studies have examined the risk for HIV transmission associated with various sex acts
(99--113). These studies indicate that some sexual behaviors do have a
lower average per-act risk for transmission than others and that
replacing a higher-risk behavior with a relatively
lower-risk behavior might reduce the likelihood that HIV transmission will occur. However, risk for HIV transmission is affected by numerous biological factors (e.g., host genetics, stage of infection, viral load, coexisting STDs) and behavioral factors (e.g., patterns of sexual and drug-injection partnering)
(105,114), and per-act risk estimates based on models that assume a
constant per-contact infectivity could be inaccurate
(110,113). Thus, estimates of the absolute per-episode risk for
transmission associated with different activities could be highly misleading when applied to a specific patient or situation. Further the relative risks of becoming infected with HIV, from the perspective of a person not infected with HIV, might vary
greatly according to the various choices related to sexual
behavior (Table 5) (115,116).
Effect of Antiretroviral Therapy on HIV Transmission.
High viral load is a major risk factor for HIV transmission
(117--125). Among untreated patients, the risk for HIV transmission through heterosexual contact has been shown to increase approximately 2.5-fold for each 10-fold increase in plasma viral load (126) (Table 6). By lowering viral
load, antiretroviral therapy might reduce risk for HIV transmission, as has been demonstrated with perinatal transmission (127,128) and indirectly suggested for transmission via genital secretions (semen and cervicovaginal fluid) (2,129--133). However, because HIV can be detected in the semen, rectal secretions, female genital secretions, and pharynx of HIV-infected patients with undetectable plasma viral loads
(16,134--137) and because consistent reduction of viral load depends on high adherence to antiretroviral regimens, the clinician should
assume that all patients who are receiving therapy, even those
with undetectable plasma HIV levels, can still transmit HIV. Patients who have treatment interruptions, whether scheduled or not, should be advised that this will likely lead to a rise in plasma viral load and increased risk for transmission. Another
concern related to adherence to antiretroviral therapy is the development of drug-resistant mutations with subsequent transmission of drug-resistant viral strains. Several reports suggest that transmission of drug-resistant HIV occurs in the United States (138--141). Recent reports suggest that drug-resistant HIV strains might be less easily transmitted than wild-type virus (142), but these data are limited and their significance is unclear.
Effectiveness of Postexposure Prophylaxis for Non occupational Exposure to HIV. Although the U.S. Public Health Service recommends
using antiretroviral drugs to reduce the likelihood of acquiring HIV infection from occupational exposure (e.g., accidental needle sticks received by health care workers) (143), limited data are available on efficacy
of prophylaxis for nonoccupational exposure
(97,143--147). Observational data suggesting effectiveness have been reported
(148); however, postexposure prophylaxis might not protect against infection in all cases, and effectiveness of these regimens might be further hindered by lack of tolerability, potential toxicity, or viral resistance. Thus, avoiding exposure remains the best
approach to preventing transmission, and the potential availability of postexposure prophylaxis should not be used as justification for engaging in risky
behavior.
Tailored Interventions for Patients at High Risk for Transmitting HIV
Interventions tailored to the individual patient's risks can be delivered to patients at highest risk for transmitting HIV infection and for acquiring new STDs. This includes patients whose risk screening indicates current sex or
drug-injection practices that may lead to transmission, who have a current or recent STD, or who have mentioned items of concern
in discussions with the clinician (149,150). Any positive results of screening for behavioral risks or STDs should be addressed in more detail with the patient so a more thorough risk assessment can be done and an appropriate risk-reduction plan can
be discussed and agreed upon.
Although the efficacy of brief clinician-delivered interventions with HIV-infected patients has not been studied
extensively, substantial evidence exists for the efficacy of provider-delivered, tailored messages for other health concerns (151--155). An attempt should be made to determine which of the patient's risk behaviors and underlying concerns can be addressed during clinic visits and which might require referral (Box 3).
At a minimum, an appropriate referral should be made and the patient should be informed of the risks involved
in continuing the behavior. HIV-infected persons who remain sexually active should be reminded that the only certain means
for preventing transmission to noninfected persons is to restrict sex to partners known to be already infected with HIV and that they have a responsibility for disclosure of HIV serostatus to prospective sex partners. For mutually consensual sex with a person of unknown or discordant HIV serostatus, consistent and correct use of condoms made of latex, polyurethane, or
other synthetic materials can substantially reduce the risk
for HIV transmission. Also, some sex acts have relatively less risk for
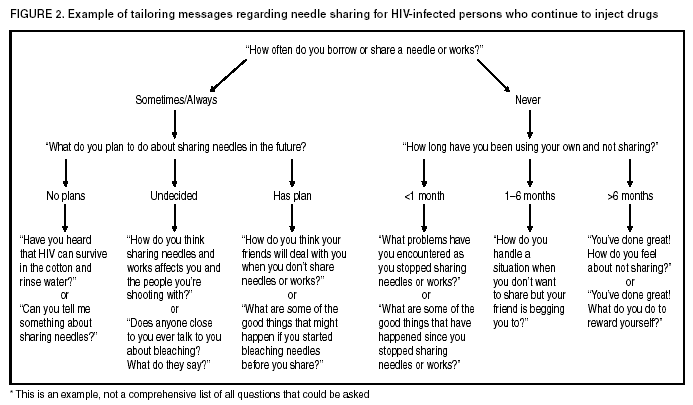
HIV transmission than others (Table 5). For HIV-infected patients who continue injection drug use, the provider should
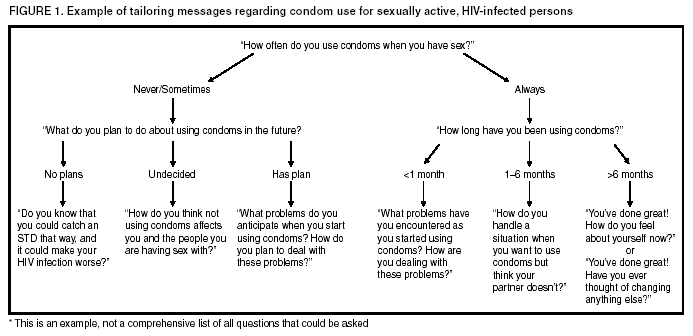
emphasize the risks associated with sharing needles and should provide information regarding substance abuse treatment and access to clean needles (Box 4) (156--158). Examples
of targeted motivational messages on condom use and needle sharing are
provided (Figures 1 and 2), and providers can individualize their own messages using these as a guide.
Clinician Training
Clinicians can prepare themselves to deliver HIV prevention messages and brief behavioral interventions to their
patients by 1) developing strategies for incorporating HIV risk-reduction interventions into patients' clinic visits
(159); 2) obtaining training on speaking with patients about sex and drug-use behaviors and on giving explanations in simple,
everyday language (68,87,160,161); 3) becoming familiar with interventions that have demonstrated effectiveness
(162); 4) becoming familiar with the underlying causes of and concerns related to risk behaviors among HIV-infected persons (e.g., domestic violence) (13,163); and 5) becoming familiar with community resources that address risk reduction. Free training on risk screening
and prevention can be obtained at CDC-funded STD/HIV Prevention Training Centers (http://depts.washington.edu/nnptc) and HRSA-funded AIDS Education and Training Centers (http://www.aids-ed.org), which also offer continuing medical education credit for this training. Ongoing training will help clinicians refine their
counseling skills as well as keep current with prevention concerns at the community level, thus increasing their ability to appropriately counsel and provide support to patients.
Ongoing Delivery of Prevention Messages
Prevention messages can be reinforced by subsequent longer or more intensive interventions in clinic or office
environments by nurses, social workers, or health educators. Advantages of a multidisciplinary approach are that skill sets vary among
staff members from various disciplines and that a patient may be more receptive to discussing prevention-related issues with one team member than with another. For HIV-negative persons or persons of unknown HIV serostatus, randomized
controlled trials provide strong evidence for the efficacy of short, one- or two-session interventions
(164--170) and for longer or multisession interventions in clinics for individuals and groups
(164,171--173). For example, for persons who continue
to engage in risky behaviors, CDC recommends client-centered counseling, a specific model of HIV prevention
counseling (44,164). Evidence for the efficacy of multisession interventions for HIV-infected patients, individually or in groups, in clinical settings is limited to a few randomized, controlled
trials (69,174,175) and other studies that might not have
assessed behavioral outcomes (6,176--180). The studies of single-session interventions for individual HIV-infected patients in clinical settings have not been randomized
controlled trials (181--187).
Referrals for Additional Prevention Interventions and Other Services
Types of Referrals
Certain patients need more intensive or ongoing behavioral interventions than can feasibly be provided in medical
care settings (44). Many have underlying problems that impede adoption of safer behaviors (e.g., homelessness, substance abuse, mental illness), and achieving behavioral change is often
dependent on addressing these concerns. Clinicians will usually
not have time or resources to fully address these issues, many of which can best be addressed through referrals for services such as intensive HIV prevention interventions (e.g., multisession risk-reduction counseling, support groups), medical services
(e.g., family planning and contraceptive counseling, substance abuse treatment), mental health services (e.g., treatment of depression, counseling for sexual compulsivity), and social services (e.g., housing, child care and custody, protection from
domestic violence). For example, all patients should be made aware of their responsibility for appropriate disclosure of HIV serostatus to sex and needle-sharing partners; however, full consideration of the complexities of disclosure, including benefits and
potential risks, may not be possible in the time available during medical visits
(188). Patients who are having, or are likely to
have, difficulty initiating or sustaining behaviors that reduce or prevent HIV transmission might benefit from prevention
case management. Prevention case management provides ongoing, intensive, one-on-one, client-centered risk assessment
and prevention counseling, and assistance accessing other services to address concerns that affect patients' health and ability to change HIV-related risk-taking behavior. For HIV-seronegative persons, randomized controlled trials provide evidence for
the efficacy of HIV prevention interventions delivered by health departments and
community-based organizations
(164,189--198). For HIV-infected persons, efficacy studies of such interventions are limited to a few
randomized controlled trials (199--201), only one of which documented change in risk-related behavior
(199), and to other studies, the majority of which did not
assess behavioral outcomes (7,202--207).
Referrals for IDUs
For IDUs, ceasing injection-drug use is the only reliable way to eliminate the risk of injection-associated HIV transmission; however, most IDUs are unable to sustain long-term abstinence without substance abuse treatment. Several studies have examined the effect of substance abuse treatment, particularly methadone maintenance treatment, on HIV risk
behaviors among IDUs (208--210). These include controlled
(211--217) and noncontrolled
(218--221) cohort studies, case-control studies
(222), and observational studies with controls (223,224), and collectively they provide evidence that
methadone maintenance treatment reduces risky injection and sexual behaviors and HIV seroconversion. Thus, early entry into substance abuse treatment programs, maintenance of treatment, and sustained abstinence from injecting are crucial for reducing the risk for HIV transmission from infected IDUs. For those IDUs not able or willing to stop injecting drugs, once-only use of
sterile syringes can greatly reduce the risk for injection-related HIV transmission. Substantial evidence from cohort, case-control, and observational studies (225) indicates that access to sterile syringes through syringe exchange programs reduces HIV
risk behavior and HIV seroconversion among IDUs. Physician prescribing and pharmacy programs can also increase access
to sterile syringes (226--231). Disinfecting
syringes and other injection equipment by boiling or flushing with bleach when
new, sterile equipment is not available has been suggested to reduce the risk for HIV transmission
(156); however, it is difficult to reliably disinfect syringes, and this practice is not as safe as using a new, sterile syringe (232--234). Information on access to sterile syringes and safe syringe disposal can be obtained through local health departments or state HIV/AIDS prevention programs.
Engaging the Patient in the Referral Process
When referrals are made, the patient's willingness and ability to accept and complete a referral should be assessed.
Referrals that match the patient's self-identified priorities are more likely to be successful than those that do not; the services need to
be responsive to the patient's needs and appropriate for the patient's culture, language, sex, sexual orientation, age,
and developmental level. For example, adolescents should be
referred to behavioral intervention programs and services that
work specifically with this population. Discussion with the patient can identify barriers to the patient's completing the referral (e.g., lack of transportation or child care, work
schedule, cost). Accessibility and convenience of services predict whether a
referral will be completed. The patient should be given
specific information regarding accessing referral services and might
need assistance (e.g., scheduling appointments, obtaining transportation) in completing referrals. The likelihood that referrals will be
completed successfully could possibly be increased
if clinicians or other health-care staff assist patients with
making appointments to referral services. When a clinician does not have the capacity to make all appropriate referrals, or when needs are especially complex, a case manager can help make referrals and coordinate care. Outreach workers, peer counselors
or educators, treatment advocates, and treatment educators can also help patients identify needs and complete referrals successfully. Health department HIV/AIDS prevention and care programs can provide information on
accessing these services. Assessing the success of referrals by documenting referrals made, the status of those referrals, and patient satisfaction
with referrals will further assist clinicians in meeting patient needs. Information obtained through
follow-up of referrals can identify barriers to completing the referral, responsiveness of referral services to patient needs, and gaps in the referral system, and can be used to develop strategies for removing the barriers.
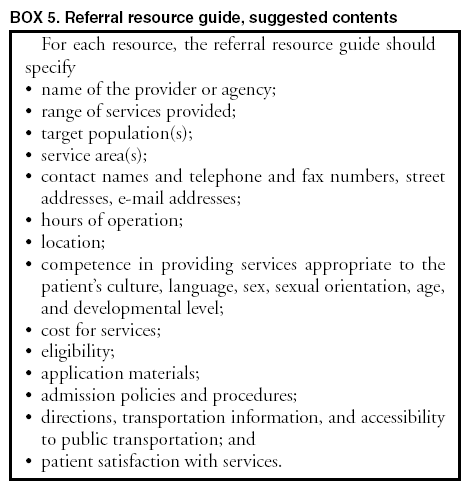
Referral Guides and Information
Preparation for making patient referrals includes 1) learning about local HIV prevention and supportive social
services, including those supported by the Ryan White CARE Act;
2) learning about available resources and having a referral
guide listing such resources; and 3) contacting staff in local programs to facilitate subsequent referrals. Referral guides and other information usually can be obtained from local and state health department HIV/AIDS prevention and care programs,
which are key sources of information about services available locally. Health departments and some managed care organizations are also a source of educational materials, posters, and other prevention-related material. Health departments can provide
or suggest sources of training and technical assistance on behavioral interventions. A complete listing of state AIDS directors and contact information is available from the National Alliance of State and Territorial AIDS Directors (NASTAD) at
http://www.nastad.org. In addition, information can be
obtained from local health planning councils, consortia, and
community planning groups; local, state, and national HIV/AIDS information hotlines and Internet websites; and community-based health and human service providers
(Box 5).
Examples of Case Situations for Prevention Counseling
1. A patient with newly diagnosed HIV infection comes to your office for initial evaluation. Of the many things that must be addressed during this initial visit (e.g., any emergent medical or psychiatric problems, education about HIV, history, physical, initial laboratory work [if not
already done]), how does one address prevention? What is the minimum that should be done, and how can it be incorporated into this visit?
Assuming no emergent issues preclude a complete history and physical examination during this visit, the following should
be done:
During the history, question how the patient might have acquired HIV, current risk behaviors, current partners
and whether they have been notified and tested for HIV, and current or past STDs.
During the physical examination, include genital and rectal examinations, evaluation and treatment of any current
STD, or, if asymptomatic, appropriate screening for STDs.
Discuss current risk behavior, at least briefly. Emphasize the importance of using condoms; address active
injection-drug use.
Discuss the need for disclosure of HIV serostatus to sex and needle-sharing partners, and discuss potential
barriers to disclosure.
Note issues that will require follow-up; e.g., risk behavior that will require continuing counseling and referral and
partners who will need to be notified by either the patient or a health department.
2. A patient with chronic, stable HIV comes to you with a new STD. What prevention considerations should
be covered in this visit?
For the patient who has had a stable course of disease, a new STD can be a sign of emerging social, emotional, or
substance abuse problems. These potential problems should be addressed in addition to the STD.
During the history, cover topics related to acquisition of the new STD---number of new partners, number of
episodes of unsafe sex, and types of unsafe sex.
Address the personal risks associated with high-risk
behavior, e.g., viral superinfection and HIV/STD interactions.
Address personal or social problems (including substance abuse and domestic violence) that might have led to a change
in behavior resulting in the acquisition of the new STD; refer to social services, if necessary.
Address other issues (e.g., adherence to HAART) that may be affected by personal or social problems. Check viral load
if nonadherence is evident or is suspected.
During the physical examination, include a careful genital and rectal examination and screen for additional STDs, such
as syphilis, trichomoniasis, (for women), chlamydial infection (for sexually active women aged
<25 years and selected populations of men and women), and gonorrhea (for selected populations of men and women).
Discuss the need for partner notification and referral for counseling and testing.
Note in the chart that risk behavior should be addressed in future visits and that tailored counseling may be needed for
the patient.
3. A patient with chronic, stable HIV has been seen regularly in a health care setting. What should be included in
this patient's routine clinical care?
Discussion of sexual and needle-sharing practices should be integrated into a routine part of clinical care.
Periodically (e.g., annually) screen for STDs. STDs to be included in screening should be determined by patient's sex, history of high-risk behavior, and local epidemiology of selected STDs.
Reiterate general prevention messages and patient education regarding partner notification, high-risk behaviors associated with transmission, prevention of transmission, or condom use, as deemed appropriate by the clinician.
4. A patient who has been treated with HAART for 2 years comes to you. At the time of treatment
initiation, CD4+count was 200 cells/µL and the viral load was 50,000 copies/ml. The response to therapy was prompt; CD4+ count increased to 500 cells/µL, and the viral load has been undetectable since soon after treatment began. The patient now has mildly elevated cholesterol, some mild lipodystrophy, and facial wasting. He states that he would like to
stop HAART because of the side effects. What should you tell this patient?
Inform the patient that upon stopping HAART,
CD4+ count and viral load will likely return to pretreatment levels with risk for opportunistic infections and progression of immune deficiency.
Inform the patient that increase in viral load to pretreatment levels will likely result in increased infectiousness and risk for transmission of HIV to sex or needle-sharing partners.
Counsel the patient regarding the option of changing the HAART regimen to limit progression of metabolic side effects.
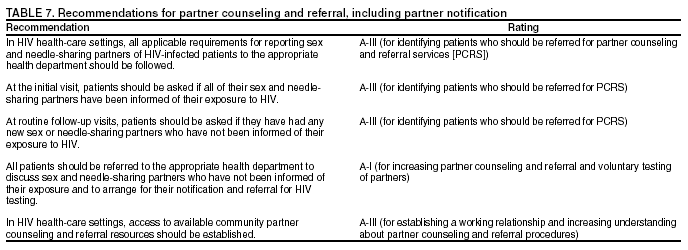
Partner Counseling and Referral Services, Including Partner Notification
HIV-infected persons are often not yet aware of their infection; thus, they cannot benefit from early medical evaluation
and treatment and do not know that they may be transmitting HIV to others. Reaching such persons as early after infection
as possible is important for their own health and is a critical strategy for reducing HIV transmission in the
community. Furthermore, interviews of HIV-infected persons in various settings suggest that >70% are sexually active after receiving their diagnosis, and many have not told their partners about their infection
(188). Partner counseling and referral services
(PCRS), including partner notification, are intended to address these problems by 1) providing services to
HIV-infected persons and their sex and needle-sharing partners so the partners can take steps to avoid becoming infected or, if already infected, to avoid infecting others and 2) helping infected partners gain earlier access to medical evaluation, treatment, and other services
(Table 7). A key element of PCRS involves informing current partners (and past partners who may have been exposed) that a
person who is HIV infected has identified them as a sex or needle-sharing partner and
advising them to have HIV counseling and testing
(235--238).
Informing partners of their exposure to HIV is confidential; i.e., partners are not told who reported their name or when
the reported exposure occurred. It is voluntary in that the
infected person decides which names to reveal to the interviewer.
Studies have indicated that infected persons are more likely to name their close partners than their more casual partners (204,239,240). Limited reports of partner violence after notification suggest a need for caution, but such violence seems to be rare (241--2). When asked, 92% of notified partners
reported that they believe the health department should continue partner
notification services (243). No studies have
directly shown that PCRS prevents disease in a community. However, studies
have demonstrated that quality HIV prevention counseling can reduce the risk of acquiring a new STD
(164) and that persons who become aware of their HIV infection can take steps to protect their health and prevent further transmission (244); in addition, before--after studies have
suggested that partners change their behavior after they are notified
(245). Finally, compelling arguments have been
offered regarding partners' rights to know this information that is important to their health.
Laws and Regulations Related to Informing Partners
The majority of states and some cities or localities have laws and regulations related to informing partners that they have
been exposed to HIV. Certain health departments require that, even if a patient refuses to report a partner, the clinician report to
the health department any partner of whom he or she is aware. Many states also have laws regarding disclosure by
clinicians to third parties known to be at high risk for future HIV transmission from patients known to be infected (i.e., duty to
warn) (246). Clinicians should know and comply with any such requirements in the areas in which they practice. With regard to PCRS, clinicians should also be aware of and adhere to all laws and regulations related to providing services to
minors.
Approaches to Notifying Partners
Partners can be reached and informed of their exposure by health department staff, clinicians in the private sector, or the infected person. In the only randomized controlled trial that has been conducted to date
(175), 35 HIV-infected persons were asked to notify their partners themselves, and 10
partners were notified. Another 39 HIV-infected persons were
assigned to health department referral; and for these, 78 partners were notified. Thus, notification by the health department appears to be substantially more effective than
notification by the infected person. Other studies, with less rigorous
designs, have demonstrated similar results
(247,248). Some persons, when asked, prefer to inform their partners themselves. This could
have a benefit if partners provide support to the infected person. However, patients frequently find that informing their partners is more difficult than they anticipated. Certain health departments offer contract referral, in which the infected person has a few days to notify his or her partners. If by the contract date the partners have not had a visit for counseling and testing, they are then contacted by the health department. In practice, patients' difficulties in
informing their partners usually means notification is done by the health department.
Although clinicians might wish to take on the responsibility for informing partners, one observational study has
indicated that health department specialists were more successful than physicians in interviewing patients and locating partners (249). Health departments have staff who are trained to do partner notification and skilled at providing this free, confidential service. These disease intervention specialists can work closely with public and private sector clinicians who treat persons with
other STDs. With regard to partner notification, the clinician should be sensitive to concerns of domestic violence or abuse by the informed partner.
All partners should be notified at least once. Persons who continue to have sex with an HIV-infected person despite an earlier notification may have erroneously concluded that someone else was the infected partner. Thus, renotification might
be important, although no research is available on renotification.
Additional information, recommendations, and requirements related to PCRS are available through health department HIV/AIDS programs. A complete listing of state AIDS directors and contact information is available from the
National Alliance of State and Territorial AIDS Directors (NASTAD) at
http://www.nastad.org.
Acknowledgments
The preparers are grateful to P. Lynne Stockton, V.M.D, and
P. Susanne Justice, CDC, for their editorial assistance and to Mark R.
Vogel, M.A., HIVMA of IDSA, who assisted in coordinating responses from members of that organization.
Janssen RS, Holtgrave DR, Valdiserri RO, Shepherd M, Gayle HD. The serostatus approach to fighting the HIV epidemic: prevention strategies
for infected individuals. Am J Public Health 2001;91:1019--24.
Institute of Medicine, Committee on HIV Prevention Strategies in the United States. No time to lose: getting more from HIV prevention. Ruiz
MS, Gable AR, Kaplan EH, Stoto MA, Fineberg HV, Trussell J, eds. Washington, DC: National Academy Press; 2001.
Chamot E, Coughlin SS, Farley TA, Rice JC. Gonorrhea incidence and HIV testing and counseling among adolescents and young adults seen
at a clinic for sexually transmitted diseases. AIDS 1999;13:971--9.
Valleroy LA, MacKellar DA, Karon JM, et al. HIV prevalence and
associated risk in young men who have sex with men. JAMA 2000;284:198--204.
Allen S, Serufilira A, Bogaerts J, et al. Confidential HIV testing and condom promotion in Africa. Impact on HIV and gonorrhea rates.
JAMA 1992;268:3338--43.
Cleary PD, Van Devanter N, Rogers TF, et al. Behavior changes after notification of HIV infection. Am J Public Health 1991;81:1586--90.
Stall RD, Hays RB, Waldo CR, Ekstrand M, McFarland W. The gay '90s: a review of research in the 1990s on sexual behavior and HIV risk
among men who have sex with men. AIDS 2000;14(suppl. 3):S101--14.
Crepaz N, Marks G. Towards an understanding of sexual risk behavior in people living with HIV: a review of social, psychological,
and medical findings. AIDS 2002;16:135--49.
Handsfield H. Resurgent STD in gay and bisexual men: a public health crisis. Presented at the 28th Annual Meeting of the Infectious Diseases
Society of America, New Orleans, Louisiana: September 7--10, 2000.
Risk reduction: sex without condoms. HIV counselor perspectives
[newsletter] Vol. 10, No. 2, March 2001.
Collis TK, Celum CL. The clinical manifestations and treatment of sexually transmitted diseases in human immunodeficiency virus--positive men.
Clin Infect Dis 2001;32:611--22.
Sheer S, Chu PL, Klausner KD, Katz MH, Schwarcz SK. Effect of highly active antiretroviral therapy on diagnoses of sexually transmitted
diseases in people with AIDS. Lancet 2001;357:432--5.
Williams LA, Klausner JD, Whittington WK. et al. Elimination and reintroduction of primary and secondary syphilis. Am J Public
Health 1999;89:1093--7.
Mayer KH, Klausner JD, Handsfield HH. Intersecting epidemics and educable moments: sexually transmitted disease risk assessment and
screening in men who have sex with men. Sex Transm Dis 2001;28:464--7.
Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice: the contribution of other sexually transmitted
diseases to sexual transmission of HIV infection. Sex Transm Infect 1999;75:3--17.
Kelly JA, Otto-Salaj LL, Sikkema KJ, Pinkerton SD, Bloom FR. Implications of HIV treatment advances for behavioral research on AIDS:
protease inhibitors and new challenges in HIV secondary prevention. Health Psychol 1998;17:310--9.
Kelly JA, Hoffman RG, Rompa D, Gray M. Protease inhibitor combination therapies and perception of gay men regarding AIDS severity and the
need to maintain safer sex. AIDS 1998;12:F91--5.
Kravcik S, Victor G, Houston S, et al. Effect of antiretroviral therapy and viral load on the perceived risk of HIV transmission and the need for
safer sexual practices. J Acquir Immune Defic Syndr Hum Retrovirol 1998;19:124--9.
Dilley JW, Woods WJ, MacFarland W. Are advances in treatment changing views about high-risk sex? [letter] N Engl J Med 1997;337:501--2.
Van de Ven P, Kippax S, Knox S, Prestage G, Crawford J. HIV treatment optimism and sexual behaviour among gay men in Sydney and
Melbourne. AIDS 1999;13:2289--94.
CDC. US HIV and AIDS cases reported through December 2000. Vol.12 (No. 2). Atlanta, GA: US Department of Health and Human
Services, CDC, 2000. Available at
http://www.cdc.gov/hiv/stats/hasr1202.htm.
Des Jarlais DC, Perlis T, Friedman SR, et al. Declining seroprevalence in a very large HIV epidemic: injecting drug users in New York City, 1991
to 1996. Am J Public Health 1998;88:1801--6.
Des Jarlais DC, Marmor M, Friedman P, et al. HIV incidence among injection drug users in New York City, 1992-1997: evidence for
a declining epidemic. Am J Public Health 2000;90:352--9.
Academy for Educational Development. A comprehensive approach: preventing blood-borne infections among injection drug users. Prepared for
CDC. Washington, DC: Academy for Educational Development, December 2000. Available at
http://www.cdc.gov/idu/idu.htm.
National Institute on Drug Abuse, Community Epidemiology Working Group (CEWG). Drug abuse highlights for the United States. 45th meeting
of the Community Epidemiology Working Group, Miami, Florida: December 15--18, 1998.
Deren S, Robles R, Andia J, Colon HM, Kang S-Y, Perlis T. Trends in HIV seroprevalence and needle sharing among Puerto Rican drug
injectors in Puerto Rico and New York: 1992--1999. J Acquir Immune Defic Syndr 2001;26:164--9.
Irwin KL, Edlin BR, Faruque S, et al. Crack cocaine smokers who turn to drug injection: characteristics, factors associated with injection,
and implications for HIV transmission. The Multicenter Crack Cocaine and HIV Infection Study Team. Drug Alcohol Depend 1996;42:85--92.
Epstein RM, Levenkron JC, Frarey L, Thompson J, Anderson K, Franks P. Improving physicians' HIV risk-assessment skills using announced
and unannounced standardized patients. J Gen Intern Med 2001;16:176--80.
Veterans Health Administration. The VA HIV prevention handbook: a guide for clinicians. Washington DC: US Department of Veterans
Affairs, Veterans Health Administration, January 2002; P95644.
National Institutes of Health. Public Health Service Task Force recommendations for the use of antiretroviral drugs in pregnant women
infected with HIV-1 for maternal health and interventions for reducing perinatal HIV-1 transmission in the United States. HIV/AIDS Treatment
Information Service (ATIS). Bethesda, MD: US Department of Health and Human Services, National Institutes of Health, 2003. Available at http://www.
http://www.aidsinfo.nih.gov/guidelines/default_db2.asp?id=66.
Wight RG, Rotheram-Borus MJ, Klosinski L, Ramos B, Calabro M, Smith R. Screening for transmission behaviors among HIV-infected adults.
AIDS Educ Prev 2000;12:431--41.
Rabin DL, Boekeloo BO, Marx ES, Bowman MA, Russell NK, Willis AG. Improving office-based physicians' prevention practices for
sexually transmitted diseases. Ann Intern Med 1994;121:513--9.
DeGuzman MA, Ross MW. Assessing the application of HIV and AIDS related education and counselling on the Internet. Patient Education
and Counseling 1999;36:209--28.
Fredman L, Rabin DL, Bowman M, et al. Primary care physicians'
assessment and prevention of HIV infection. Am J Prev Med 1989;5:188--95.
Orlander JD, Samet JH, Kazis L, Freeberg KA Libman H. Improving medical residents' attitudes toward HIV-infected persons through training in
an HIV staging and triage clinic. Acad Med 1994;69:1001--3.
Sullivan L, Stein MD, Savetsky, JB, Samet JH. The doctor--patient
relationship and HIV-infected patients' satisfaction with primary care physicians. J Gen Intern Med 2000;15:462--9.
Boekeloo BO, Schiavo L, Rabin DL, Conlon RT, Jordan CS, Mundt DJ. Self-reports of HIV risk factors by patients at a sexually transmitted
disease clinic: audio vs. written questionnaires. Am J Public Health 1994; 84:754--60.
Webb PM, Zimet GD, Fortenberry JD, Blythe MJ. Comparability of a computer-assisted versus written method for collecting health
behavior information from adolescent patients. J Adolesc Health 1999;24:383--8.
Kissinger P, Rice J, Farley T, et al. Application of computer-assisted
interviews to sexual behavior research. Am J Epidemiol 1999;149:950--4.
California STD Controllers Association, California Coalition of Local AIDS Directors. Guidance for STD clinical preventive services
for persons infected with HIV. Sex Transm Dis 2001;28:460--3.
Metzger DS, Koblin B, Turner C, et al. Randomized controlled trial of audio computer-assisted self-interviewing: utility and acceptability
in longitudinal studies. HIVNET Vaccine Preparedness Study Protocol Team. Am J Epidemiol 2000;152:99--106.
Mofenson LM, McIntyre JA. Advances and research directions in the prevention of mother-to-child HIV-1 transmission. Lancet 2000;355:2237--44.
Duggan J, Walerius H, Purohit A, et al. Reproductive issues in HIV-seropositive women: a survey regarding counseling, contraception, safer sex,
and pregnancy choices. J Assoc Nurses AIDS Care 1999;10:84--92.
Ethics Committee of the American Society of Reproductive Medicine. Human immunodeficiency virus and infertility treatment. Fertil
Steril 2002;77:218--22.
Hopkins DP, Briss PA, Ricard CJ, et al. Reviews of evidence regarding interventions to reduce tobacco use and exposure to
environmental tobacco smoke. Am J Prev Med 2001;20(2 suppl):16--66.
Scholes D, Anderson LA, Operskalski B, BlueSpruce J, Irwin K, Magid DJ. The role of managed care in STD prevention and control.
Washington, DC: American Association of Health Plans, 1999.
Kaplan JE, Masur H, Holmes KK, et al. An overview of the 1999 US Public Health Service/Infectious Diseases Society of America guidelines
for preventing opportunistic infections in human immunodeficiency virus--infected persons. Clin Infect Dis 2000;30(suppl 1):S15--28.
STD Control Program and the HIV/AIDS Control Program, Public Health -- Seattle & King County. Sexually transmitted disease and HIV
screening guidelines for men who have sex with men. Sex Transm Dis 2001;28:457--9.
Dodge WT, BlueSpruce J, Grothaus L, et al. Enhancing primary care HIV prevention: a comprehensive clinical intervention. Am J Prev
Med 2001;20:177--83.
Kalichman SC, Rompa D, Cage M, et al. Effectiveness of an intervention to reduce HIV transmission risks in HIV-positive people. Am J Prev
Med 2001;21:84--92.
Grosskurth H, Mosha F, Todd J, et al. Impact of improved treatment of sexually transmitted diseases on HIV infection in rural Tanzania:
randomised controlled trial. Lancet 1995;346:530--6.
Wasserheit JN. Epidemiological synergy: interrelationships between
human immunodeficiency virus infection and other sexually
transmitted diseases. Sex Transm Dis 1992;19:61--77.
Cohen MS. Sexually transmitted diseases enhance HIV transmission: no longer a hypothesis. Lancet 1998;351(suppl 3):5--7.
Quinn TC. Association of sexually transmitted diseases and infection with the human immunodeficiency virus: biological cofactors and markers
of behavioural interventions. Int J STD AIDS 1996;7(suppl 2):17--24.
Kamb ML, Newman D, Peterman TA, et al. Most bacterial STD are asymptomatic. [Abstract 266] In: Abstracts of STIs at the Millennium,
Past, Present, and Future -- A Joint Meeting of the ASTDA and the MSSVD,
Baltimore, Maryland, May 2000.
Phillips RS, Hanff PA, Wertheimer A, Aronson MD. Gonorrhea in women seen for routine gynecologic care: criteria for testing. Am J
Med 1988;85:177--82.
Schachter J, Stoner E, Moncada J. Screening for chlamydial infections
in women attending family planning clinics. West J Med 1983;138:375--9.
Handsfield HH, Lipman TO, Harnisch JP, Tronca E, Holmes KK.
Asymptomatic gonorrhea in men. Diagnosis, natural course, prevalence,
and significance. N Engl J Med 1974;290:117--23.
Alexander-Rodriguez T, Vermund SH. Gonorrhea and syphilis in incarcerated urban adolescents: prevalence and physical signs. Pediatrics
1987;80:561--4.
Ellerbeck EF, Vlahov D, Libonati JP, Salive ME, Brewer TF. Gonorrhea
prevalence in the Maryland state prisons. Sex Transm Dis 1989;16:165--7.
Grosskurth H, Mayaud P, Mosha F, et al. Asymptomatic gonorrhea and chlamydial infection in rural Tanzanian men. BMJ 1996;312:277--80.
Mehta SD, Rothman RE, Kelen GD, Quinn TC, Zenilman JM.
Unsuspected gonorrhea and chlamydia in patients of an urban adult
emergency department: a critical population for STD control intervention. Sex Transm Dis 2001;28:33--9.
American Academy of Pediatrics, Committee on Pediatric AIDS and Committee on Adolescence. Adolescents and human immunodeficiency
virus infection: the role of the pediatrician in prevention and intervention. Pediatrics 2001;107:188--90.
Rost K, Nutting PA, Smith J, Werner JJ. Designing and implementing a primary care intervention trial to improve the quality and outcome of care
for major depression. Gen Hosp Psychiatry 2000;22:66--77.
Hollis JF, Lichtenstein, E, Vogt TM, Stevens VJ, Biglan A.
Nurse-assisted counseling for smokers in primary care. Ann Intern Med 1993;118:521--5.
Stevens VJ, Severson H, Lichtenstein E, Little SJ, Leben J. Making the most of a teachable moment: a smokeless-tobacco cessation intervention in
the dental office. Am J Public Health 1995; 85:231--5.
Cornuz J, Zellweger JP, Mounoud C, Decrey H, Pecoud A, Burnand B. Smoking cessation counseling by residents in an outpatient clinic. Prev
Med 1997;26:292--6.
Hartmann KE, Thorp JM, Pahel-Short L, Koch MA. A randomized controlled trial of smoking cessation intervention in pregnancy in an
academic clinic. Obstet Gynecol 1996;87:621--6.
Ockene, JK, Kristeller J, Goldberg R, et al.. Increasing the efficacy of physician-delivered smoking interventions: a randomized clinical trial. J
Gen Intern Med 1991;6:1--8.
Ockene JK, Kristeller J, Pbert L, et al. The physician-delivered smoking intervention project: can short-term interventions produce long-term
effects for a general outpatient population? Health Psychol 1994;13:278--81.
Ockene JK, Adams A, Hurley TG, Wheeler EV, Hebert JR. Brief
physician- and nurse practitioner-delivered counseling for high-risk drinkers: does it work? Arch Intern Med 1999;159:2198-205.
Senft RA, Polen MR, Freeborn DK, Hollis JF. Brief intervention in a primary care setting for hazardous drinkers. Am J Prev Med 1997;13:464--70.
Ockene IS, Hebert JR, Ockene JK, et al. Effect of physician-delivered nutrition counseling training and an office-support program on saturated
fat intake, weight, and serum lipid measurements in a hyperlipidemic population: Worcester Area Trial for Counseling in Hyperlipidemia
(WATCH). Arch Intern Med 1999;159:725--31.
Calfas KJ, Long BJ, Sallis JF, Wooten WJ, Prall M, Patrick K. A
controlled trial of physician counseling to promote the adoption of physical
activity. Prev Med 1996;25:225--33.
Jost S, Bernard M-C, Kaiser L, et al. A patient with HIV-1 superinfection. N Engl J Med 2002;347:731--6.
Ramos A, Hu DJ, Nguyen L, et al. Intersubtype human immunodeficiency virus type 1 superinfection following seroconversion to primary
infection in two injection drug users. J Virol 2002;76:7444--52.
Essien EJ, Meshack AF, Ross MW. Misperceptions about HIV transmission among heterosexual African-American and Latino men and women.
J Natl Med Assoc 2002;94:304--12.
Peterman TA, Stoneburner RL, Allen JR, Jaffe HW, Curran JW. Risk of human immunodeficiendy virus transmission from heterosexual adults
with transfusion-associated infections. JAMA 1988;259:55--8.
DeGruttola V, Seage GR III, Mayer KH, Horsburgh CR Jr. Infectiousness of HIV between male homosexual partners. J Clin Epidemiol
1989;42:849--56.
Johnson AM, Petherick A, Davidson SJ, et al. Transmission of HIV to heterosexual partners of infected men and women. AIDS 1989;3:367--72.
Laga M, Taelman H, Van der Stuyft P, Bonneux L, Vercauteren G, Piot P. Advanced immunodeficiency as a risk factor for heterosexual transmission
of HIV. AIDS 1989;3:361--6.
Wiley JA, Herschkorn SJ, Padian NS. Heterogeneity in the probability of HIV transmission per sexual contact: the case of
male-to-female transmission in penile-vaginal intercourse. Stat Med 1989;8:93--102.
Padian NS, Shiboski SC, Jewell NP. Female-to-male transmission of human immunodeficiency virus. JAMA 1991;266:1664--7.
European Study Group on Heterosexual Transmission of HIV. Comparison of female to male and male to female transmission of HIV in 563
stable couples. BMJ 1992;304:809--13.
Saracco A, Musicco M, Nicolosi A, et al. Man-to-woman sexual transmission of HIV: longitudinal study of 343 steady partners of infected men.
J Acquir Immune Defic Syndr 1993;6:497--502.
De Vincenzi I. A longitudinal study of human immunodeficiency
virus transmission by heterosexual partners. N Engl J Med 1994;331:341--6.
Nicolosi A, Correa Leite ML, Musicco M, Arici C, Gavazzeni G, Lazzarin A. The efficiency of male-to-female and female-to-male sexual
transmission of the human immunodeficiency virus: a study of 730 stable couples. Italian Study Group on HIV Heterosexual Transmission.
Epidemiology 1994;5:570--5.
Nicolosi A, Musicco M, Saracco A, Lazzarin A. Risk factors for woman-to-man sexual transmission of the human immunodeficiency virus.
Italian Study Group on Heterosexual Transmission. J Acquir Immune Defic Syndr 1994;7:296--300.
Downs AM, De Vincenzi I. Probability of heterosexual transmission of HIV: relationship to the number of unprotected sexual
contacts. J Acquir Immune Defic Syndr Hum Retrovirol 1996;11:388--95.
Padian NS, Shiboski SC, Glass SO, Vittinghoff E. Heterosexual transmission of human immunodeficiency virus in Northern California: results
from a ten-year study. Am J Epidemiol 1997;146:350--7.
Leynaert B, Downs AM, De Vincenzi I. Heterosexual transmission of human immunodeficiency virus: variability of infectivity throughout the
course of infection. European Study Group on Heterosexual Transmission of HIV. Am J Epidemiol 1998;148:88--96.
Vittinghoff E, Douglas J, Judson F, McKirnan D, MacQueen K, Buchbinder SP . Per-contact risk of human immunodeficiency transmission
between male sexual partners. Am J Epidemiol 1999;150: 308--11.
Royce RA, Sena A, Cates W Jr, Cohen MS. Sexual transmission of HIV. N Engl J Med 1997;336:1072--8.
Varghese B, Maher JE, Peterman TA, Branson BM, Steketee RW.
Reducing the risk of sexual HIV transmission: quantifying the per-act risk for
HIV on the basis of choice of partner, sex act, and condom use. Sex Transm Dis 2002;29:38--43.
Macaluso JM, Kelaghan J, Artz L, et al. Mechanical failure of the latex condom in a cohort of women at high STD risk. Sex Transm Dis
1999;26:450--8.
Schaffer N, Roongpisuthipong A, Siriwasin W, et al. Maternal virus load and perinatal human immunodeficiency virus type 1, subtype
E transmission, Thailand. Bangkok Collaborative Perinatal HIV
Transmission Study Group. J Infect Dis 1999;179:590--9.
Mofenson LM, Lambert JS, Stiehm ER, et al. Risk factors for perinatal transmission of human immunodeficiency virus type 1 in women treated
with zidovudine. Pediatric AIDS Clinical Trials Group Study 185 Team. N Engl J Med 1999;341:385--93.
Garcia PM, Kalish LA, Pitt J, et al. Maternal levels of plasma human immunodeficiency virus type 1 RNA and the risk of perinatal
transmission. Women and Infants Transmission Study Group. N Engl J Med 1999;341:394--402.
Busch MP, Operskalski EA, Mosley JW, et al. Factors influencing
human immunodeficiency virus type 1 transmission by blood
transfusion. Transfusion Safety Study Group. J Infect Dis 1996;174:26--33.
Operskalski EA, Stram DO, Busch MP, et al. Role of viral load in heterosexual transmission of human immunodeficiency virus type 1 by
blood transfusion recipients. Am J Epidemiol 1997;146:655--61.
Lee T-H, Sakahara N, Fiebig E, Busch MP, O'Brien TR, Herman SA. Correlation of HIV-1 RNA levels in plasma and heterosexual transmission
of HIV-1 from infected transfusion recipients. J Acquir
Immune Defic Syndr Hum Retrovirol 1996;12:427--8.
Gray RH, Wawer MJ, Brookmeyer R, et al. Probability of HIV-1
transmission per coital act in monogamous, heterosexual,
HIV-1-discordant couples in Rakai, Uganda. Lancet 2001;357:1149--53.
Chakraborty H, Sen PK, Helms RW, et al. Viral burden in genital secretions determines male-to-female sexual transmission of HIV-1: a
probabilistic empiric model. AIDS 2001;15:621--7.
Quinn TC, Wawer MJ, Sewankambo N, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project
Study Group. N Engl J Med 2000;342:921--9.
Sperling RS, Shapiro DE, Coombs RW, et al. Maternal viral load, zidovudine treatment and the risk of transmission of human
immunodeficiency virus type 1 from mother to infant. Pediatric AIDS Clinical Trials Group Protocol 076 Study Group. N Engl J Med 1996;335:1621--9.
Schaffer N, Chuachoowong R, Mock PA, et al. Short-course zidovudine for perinatal HIV-1 transmission in Bangkok, Thailand: a
randomised controlled trial. Bangkok Collaborative Perinatal HIV Transmission Study Group. Lancet 1999;353:773--80.
Ghys PD, Fransen K, Diallo MO, et al. The associations between cervicovaginal HIV shedding, sexually transmitted diseases
and immunosuppression in female sex workers in Abidjan, Côte d'Ivoire. AIDS 1997;11:F85--93.
Gupta P, Mellors J, Kingsley L, et al. High viral load in semen of
human immunodeficiency virus type 1--infected men at all stages of disease and
its reduction by therapy with protease and nonnucleoside reverse transcriptase inhibitors. J Virol 1997;71:6271--5.
Vernazza PL, Gilliam BL, Dyer J, et al. Quantification of HIV in
semen: correlation with antiviral treatment and immune status. AIDS
1997;11:987--93.
Vernazza PL, Gilliam BL, Flepp M, et al. Effect of antiviral treatment on the shedding of HIV-1 in semen. AIDS 1997;11:1249--54.
Chuachoowong R, Shaffer N, Siriwasin W, et al. Short-course antenatal zidovudine reduces both cervical human immunodeficiency virus type 1
levels and risk of perinatal transmission. Bangkok Collaborative
Perinatal HIV Transmission Study Group. J Infect Dis 2000;181:99--106.
Zhang H, Dornadula G, Beumont M, et al. Human immunodeficiency virus type 1 in the semen of men receiving highly active antiretroviral
therapy. N Engl J Med 1998;339:1803--9.
Kiviat NB, Critchlow CW, Hawes SE, et al. Determinants of human immunodeficiency virus DNA and RNA shedding in the anal-rectal canal
of homosexual men. J Infect Dis 1998;177:571--8.
Lampinen TM, Critchlow CW, Kuypers JM, et al. Association of antiretroviral therapy with detection of HIV-1 RNA and DNA in the
anorectal mucosa of homosexual men. AIDS 2000;14:F69--75.
Kovacs A, Wasserman SS, Burns D, et al. Determinants of HIV-1 shedding in the genital tract of women. WIHS Study Group.
Lancet 2001;358:1593--601.
Little SJ, Daar ES, D'Aquila RT, et al. Reduced antiretroviral drug susceptibility among patients with primary HIV infection. JAMA
1999;282:1142--9.
Boden D, Hurley A, Zhang L, et al. HIV-1 drug resistance in newly infected individuals. JAMA 1999;282:1135--41.
Little SJ. Transmission and prevalence of HIV resistance among treatment-naive subjects. Antivir Ther 2000;5:33--40.
Little SJ, Holte S, Routy JP, et al. Antiretroviral-drug resistance among patients recently infected with HIV. N Engl J Med 2002;347:385--94.
Blower SM, Aschenbach AN, Gershengorn HB, Kahn JO. Predicting the unpredictable: transmission of drug-resistant HIV. Nat Med
2001;7:1016--20.
Katz MH, Gerberding JL. Postexposure treatment of people exposed to human immunodeficiency virus through sexual contact or
injection-drug use. N Engl J Med 1997;336:1097--100.
Katz MH, Gerberding JL. The care of persons with recent sexual
exposure to HIV. Ann Intern Med 1998:128:306--12.
Bamberger JD, Waldo CR, Gerberding JL, Katz MH. Postexposure prophylaxis for human immunodeficiency virus (HIV) infection
following sexual assault. Am J Med 1999;106:323--6.
Wiebe ER, Comay SE, McGregor M, Ducceschi S. Offering HIV
prophylaxis to people who have been sexually assaulted: 16 months' experience in
a sexual assault service. CMAJ: Canadian Medical Association
Journal 2000;162:641--5.
Schecter M, Lago RF, Ismerio R, Mendelsohn AB, Harrison LH.
Acceptability, behavioral impact, and possible efficacy of
post-sexual-exposure chemoprophylaxis (PEP) for HIV. [Abstract 15]. Presented at the 9th Conference on Retroviruses and Opportunistic Infections. Seattle, Washington, February 2002.
Coury-Doniger P, Levenkron JC, Knox KL, Cowell S, Urban MA. Use of stage of change (SOC) to develop an STD/HIV behavioral
intervention: phase 1. A system to classify SOC for STD/HIV sexual risk behaviors---development and reliability in an STD clinic. AIDS
Patient Care & STDs 1999;13:493--502.
Temmerman M, Moses S, Kiragu D, et al. Impact of single session post-partum counselling of HIV infected women on their subsequent
reproductive behaviour. AIDS Care 1990;2:247--52.
Bien TH, Miller WR, Tonigan JS. Brief interventions for alcohol
problems: a review. Addiction 1993; 88:315--35.
Campbell MK, DeVellis BM, Strecher VJ, Ammerman AS, DeVellis RF, Sandler RS. Improving dietary behavior: the effectiveness of
tailored messages in primary care settings. Am J Public Health 1994;84:783--7.
Goldberg DN, Hoffman AM, Farinha MF, et al. Physician delivery of smoking-cessation advice based on the stages-of-change model. Am J Prev
Med 1994;10:267--74.
Rakowski W, Ehrich B, Goldstein MG, et al. Increasing mammography among women aged 40--74 by use of stage-matched, tailored
intervention. Prev Med 1998;27:748--56.
Saunders B, Wilkinson C, Phillips M. The impact of a brief motivational intervention with opiate users attending a methadone programme. Addiction 1995;90:415--24.
US Department of Health and Human Services. Medical advice for persons who inject illicit drugs. HIV Prevention Bulletin. CDC; Health
Resources and Services Administration; National Institute on Drug Abuse, National Institutes of Health; Substance Abuse and Mental Health
Services Administration; May 1997. Available at
http://www.cdc.gov/idu/pubs/hiv_prev.htm.
Academy for Educational Development. A comprehensive approach: preventing blood-borne infections among injection drug users.
Washington, DC: Academy for Educational Development; 2001.
Prepared for the CDC. Available at
http://www.cdc.gov/idu/pubs/ca/comprehensive-approach.htm.
CDC National Prevention Information Network. HIV Connect, Vol. 11, No. 8. Available at
http://www.cdcnpin.org.
Fisher WA, Fisher JD, Friedland G, Cornman D, Amico R. The
Options Project: a physician-delivered intervention for HIV+ individuals in clinical care settings. [Abstract 249]. Presented at the 2001
National HIV Prevention Conference. Atlanta, Georgia, August, 2001.
DePoy E, Burke JP, Sherwen L. Training trainers: evaluating services provided to children with HIV and their families. Research on Social
Work Practice 1992;2:39--55.
Levinson W, Cohen MS, Brady D, Duffy FD. To change or not to change: "sounds like you have a dilemma." Ann Intern Med 2001;135:386--91.
CDC. Compendium of HIV prevention interventions with evidence of effectiveness. Atlanta, Georgia: US Department of Health
and Human Services, CDC; 1999 (Revised 2001). Available at
http://www.cdc.gov/hiv/pubs/HIVcompendium/hivcompendium/pdf.
Collins C, Morin SD, Shriver MD, Coates TJ. Designing primary
prevention for people living with HIV. [Policy monograph]. San
Francisco: AIDS Research Institute, University of California, San Francisco, 2000. Available at
http://ari.ucsf.edu/pdf/PrimaryPrevention.pdf.
Kamb ML, Fishbein M, Douglas JM Jr., et al., Project RESPECT Study Group. Efficacy of risk-reduction counseling to prevent
human immunodeficiency virus and sexually transmitted diseases: a randomized controlled trial. JAMA 1998;280:1161--7.
Mansfield CJ, Conroy ME, Emans SJ, Woods ER. Pilot study of AIDS education and counseling of high-risk adolescents in an office setting.
J Adolesc Health 1993; 14:115--9.
O'Donnell CR, O'Donnell L, San Doval A, Duran R, Labes K.
Reductions in STD infections subsequent to an STD clinic visit.
Using video-based patient education to supplement provider interactions. Sex Transm Dis 1998;25:161--8.
O'Donnell L, San Doval A, Duran R, O'Donnell CR. The effectiveness of video-based interventions in promoting condom acquisition among
STD clinic patients. Sex Transm Dis 1995;22:97--103.
Cohen D, Dent C, MacKinnon D. Condom skills education and
sexually transmitted disease reinfection. J Sex Res 1991;28:139--44.
Cohen DA, MacKinnon DP, Dent C, Mason HR, Sullivan E. Group counseling at STD clinics to promote use of condoms. Public Health
Rep 1992;107:727--31.
Wenger NS, Greenberg JM, Hilborne LH, Kusseling F, Mangotich M, Shapiro MF. Effect of HIV antibody testing and AIDS education
on communication about HIV risk and sexual behavior. A randomized, controlled trial in college students. Ann Intern Med 1992;117:905--11.
Hobfoll SE, Jackson AP, Lavin J, Britton P, Shepherd JB. Reducing inner-city women's AIDS risk activities: a study of single, pregnant women.
Health Psychol 1994;13:397--403.
Kelly JA, St. Lawrence JS, Hood HV, Brasfield TL. Behavioral intervention to reduce AIDS risk activities. J Consult Clin Psychol 1989;57:60--7.
Kelly JA, Murphy DA, Washington CD, et al. The effects of HIV/AIDS intervention groups for high-risk women in urban clinics. Am J
Public Health 1994;84:1918--22.
Grella CD, Annon JJ, Anglin MD. Ethnic differences in HIV risk
behaviors, self-perceptions, and treatment outcomes among women in
methadone maintenance treatment. J Psychoactive Drugs 1995;27:421--33.
Landis SE, Schoenbach VJ, Weber DJ, et al. Results of a randomized trial of partner notification in cases of HIV infection in North
Carolina. N Engl J Med 1992;326:101--6.
Lie GT, Biswalo PM. HIV-positive patient's choice of a significant other to be informed about the HIV-test result: findings from an
HIV/AIDS counselling programme in the regional hospitals of Arusha and Kilimanjaro, Tanzania. AIDS Care 1996;8:285--96.
Müller O, Sarangbin S, Ruxrungtham K, Sittitrai W, Phanuphak P. Sexual risk behaviour reduction associated with voluntary HIV counselling
and testing in HIV infected patients in Thailand. AIDS Care 1995;7:567--72.
Allen S, Serufilira A, Gruber V, et al. Pregnancy and contraception use among Rwandan women after HIV testing and counseling. Am J
Public Health 1993;83:705--10.
Fawzy FI, Namir S, Wolcott DL. Structured group intervention model for AIDS patients. Psychiatr Med 1989;7:35--45.
Hedge B, Glover LF. Group intervention with HIV seropositive
patients and their partners. AIDS Care 1990;2:147--54.
Hjorther A, Nielsen FM, Segest E. Prevention of AIDS: free condoms to drug abusers in the municipality of Copenhagen. Int J
Addictions 1990;25:745--53.
Guydish J, Temoshok L, Dilley J, Rinaldi J. Evaluation of a hospital based substance abuse intervention and referral service for HIV
affected patients. Gen Hosp Psychiatry 1990;12:1--7.
Rao AV, Swaminathan R, Baskaran S, Belinda C, Andal G, Saleem K. Behaviour change in HIV infected subjects following health education. Indian
J Med Res 1991;93:345--9.
Ryder RW, Batter VL, Nsuami M, et al. Fertility rates in 238 HIV-1 seropositive women in Zaire followed for 3 years post-partum.
AIDS 1991;5:1521--7.
Ladner J, Leroy V, Msellati P, et al. Cohort study of factors associated with failure to return for HIV post-test counselling in pregnant women:
Kigali, Rwanda, 1992--1993. AIDS 1996;10:69--75.
Pickering J, Quigley M, Pepin J, Todd J, Wilkins A. Effects of post-test counselling on condom use among prostitutes in The Gambia.
AIDS 1993;7:271--3.
Marks G, Burris S, Peterman TA. Reducing sexual transmission of HIV from those who know they are infected: the need for personal and
collective responsibility. AIDS 1999;13:297--306.
Des Jarlais DC, Casriel C, Friedman SR, Rosenblum A. AIDS and the transition to illicit drug injection---results of a randomized
trial prevention program. British Journal of Addiction 1992;87:493--8.
DiClemente RJ, Wingood GM. A Randomized controlled trial of an HIV sexual risk-reduction intervention for young African-American
women. JAMA 1995;274:1271--6.
El-Bassel N, Schilling RF. 15-month followup of women methadone patients taught skills to reduce heterosexual HIV transmission. Public
Health Rep 1992;107:500--4.
Jemmott JB, III, Jemmott LS, Fong GT. Reductions in HIV
risk-associated sexual behaviors among black male adolescents: effects of an AIDS prevention intervention. Am J Public Health 1992;82:372--7.
McCusker J, Stoddard AM, Zapka JG, Morrison CS, Zorn M, Lewis BF. AIDS education for drug abusers: evaluation of short-term
effectiveness. Am J Public Health 1992;82:533--40.
Rotheram-Borus M, Van Rossem R, Lee M, et al. Reductions in HIV risk among runaway youths. Prevention Science. In press, 2003.
Shain RN, Piper JM, Newton ER, et al. A randomized, controlled trial of a behavioral intervention to prevent sexually transmitted disease
among minority women. N Engl J Med 1999;340:93--100.
Stanton BF, Li X, Ricardo I, Galbraith J, Feigelman S, Kaljee L. A randomized, controlled effectiveness trail of an AIDS prevention program for
low-income African-American youths. Arch Pediatr Adolesc Med 1996;150:363--72.
St. Lawrence JS, Brasfield TL, Jefferson KW, Alleyne E, O'Bannon RE, III, Shirley A. Cognitive-behavioral intervention to reduce
African-American adolescents' risk for HIV infection. J Consult Clin Psychol 1995;63:221--37.
Wenger NS, Linn LS, Epstein M, Shapiro MF. Reduction of high-risk sexual behavior among heterosexuals undergoing HIV antibody testing:
a randomized clinical trial. Am J Public Health 1991;81:1580--5.
Valdiserri RO, Lyter DW, Leviton LC, Callahan CM, Kingsley LA, Rinaldo CR. AIDS prevention in homosexual and bisexual men:
results of a randomized trial evaluating two risk reduction interventions. AIDS 1989;3:21--6.
Coates TJ, McKusick L, Kuno R, Stites DP. Stress reduction training changed number of sexual partners but not immune function in men with
HIV. Am J Public Health 1989;79:885--7.
Kelly JA, Murphy DA, Bahr GR, et al. Outcome of
cognitive-behavioral and support group brief therapies for depressed, HIV-infected persons. Am J Psychiatry 1993;150:1679--86.
Darrow WW, Webster RD, Kurtz SP, Buckley AK, Patel KI, Stempel RR. Impact of HIV counseling and testing on HIV-infected men who have
sex with men: the South Beach Health Survey. AIDS and
Behavior 1998;2:115--26.
Parsons JT, Huszti HC, Crudder SO, Rich L, Mendoza J. Maintenance of safer sexual behaviors: evaluation of a theory based intervention for
HIV seropositive men with haemophilia and their female partners. Haemophilia 2000;6:181--90.
Perry SW, Card CA, Moffatt M, Ashman T, Fishman B, Jacobsberg LB. Self-disclosure of HIV infection to sexual partners after repeated
counseling. AIDS Educ Prev 1994;6:403--11.
Pomeroy EC, Rubin A, Van Lamingham L, Walker RJ. "Straight Talk": the effectiveness of a psychoeducational group intervention for
heterosexuals with HIV/AIDS. Research on Social Work Practice 1997;7: 149--64.
Turnbull PJ, Dolan KA, Stimson GV. HIV testing, and the care and treatment of HIV positive people in English prisons. AIDS Care
1993;5:199--206.
Wong-Rieger D, David L. Causal evaluation of impact of support workshop for HIV+ men. Can J Public Health 1993;84(suppl 1):S66--70.
Gibson DR, Flynn NM, McCarthy JJ. Effectiveness of methadone treatment in reducing HIV risk behavior and HIV seroconversion among
injecting drug users. AIDS 1999;13:1807--18.
National Institutes of Health (NIH) Consensus Development Program. Effective medical treatment of opiate addiction. NIH Consensus
Statement Online. 1997 Nov 17--19;15(6):1--38. Available at
http://odp.od.nih.gov/consensus/cons/108/108_statement.htm.
National Institute on Drug Abuse. Principles of drug addiction treatment: a research-based guide. Rockville, MD: US Department of Health
and Human Services, National Institutes of Health, National Institute on Drug Abuse,1999; NIH Publication No. 99-4180.
Ball JC, Lange WR, Meyers CP, Friedman SR. Reducing the risk of AIDS through methadone maintenance treatment. J Health Soc
Behav 1988;29:214--26.
Metzger DS, Woody GE, McLellan AT, et al. Human immunodeficiency virus seroconversion among intravenous drug users in- and out-of
treatment: an 18-month prospective follow-up. J Acquir Immune Defic Syndr 1993;6:1049--56.
Moss AR, Vranizian K, Gorter R, Bacchetti P, Watters J, Osmond D. HIV serocoversion in intravenous drug users in San Francisco,
1985--1990. AIDS 1994;8:223--31.
Neaigus A, Sufian M, Friedman SR, et al. Effects of an outreach intervention on risk reduction among intravenous drug users. AIDS Educ
Prev 1990;2:253--71.
Shore RE, Marmor M, Titus S, Des Jarlais DC. Methadone maintenance and other factors associated with intraindividual temporal trends
in injection-drug use. J Subst Abuse Treat 1996;3:241--8.
Wells EA, Calsyn DA, Clark LL, Saxon AJ, Jackson TR. Retention in methadone maintenance is associated with reductions in different HIV
risk behaviors for women and men. Am J Drug Alcohol Abuse 1996;22:509--21.
Zangerle R, Fuchs D, Rossler H, et al. Trends in HIV infection among intravenous drug users in Innsbruck, Austria. J Acquir Immune Defic
Syndr 1992;5:865--71.
Condelli WS, Dunteman GH. Exposure to methadone programs and heroin use. Am J Drug Alcohol Abuse 1993;19:65--78.
Greenfield L, Biglow GE, Brooner RK. Validity of intravenous drug abusers' self-reported changes in HIV high-risk drug use behaviors. Drug
Alcohol Depend 1995;39:91--8.
Martin GS, Serpelloni G, Galvan V, et al. Behavioural change in
injecting drug users: evaluation of an HIV/AIDS education programme. AIDS
Care 1990;2:275--9.
Watkins KE, Metzger D, Woody G, McLellan AT. High-risk sexual behaviors of intravenous drug users in- and out-of-treatment: implications for
the spread of HIV infection. Am J Drug Alcohol Abuse 1992;18:389--98.
Serpelloni G, Carrieri MP, Rezza G, Morganti S, Gomma M, Binkin N. Methadone treatment as a determinant of HIV risk reduction
among injecting drug users: a nested case controlled study. AIDS Care 1994;6:215--20.
Baker A, Kochan N, Dixon J, Wodak A, Heather N. HIV risk-taking behaviour among injecting drug users currently, previously and never enrolled
in methadone treatment. Addiction 1995;90:545--54.
Capelhorn JR, Ross MW. Methadone maintenance and the likelihood of risky needle sharing. Int J Addictions 1995;30:685--98.
Gibson DR, Flynn NM, Perales D. Effectiveness of syringe exchange programs in reducing HIV risk behavior and HIV seroconversion
among injecting drug users. AIDS 2001;15:1329--41.
Academy for Educational Development. Access to sterile syringes.
Washington, DC; June 2000. Prepared for CDC. Available at
http://www.cdc.gov/idu.
Cotten-Oldenburg NU, Carr P, DeBoer JM, Collison EK, Novotny G. Impact of pharmacy-based syringe access on injection practices
among injecting drug users in Minnesota. J Acquir Immune Defic Syndr 2001;27:183--92.
Gleghorn AA, Wright-De Aguero L, Flynn C. Feasibility of one-time use of sterile syringes: a study of active injection drug users in seven
United States metropolitan areas. J Acquir Immune Defic Syndr Hum Retrovirol 1998;18(suppl 1):S30--6.
Burris S, Lurie P, Abrahamson D, Rich JD. Physician prescribing of sterile injection equipment to prevent HIV infection: time for action. Ann
Intern Med 2000;133:218--26.
Rich JD, Macalino GE, McKenzie M, Taylor LE, Burris S. Syringe prescription to prevent infection in Rhode Island: a case study. Am J Public
Health 2001;91:699--700.
Groseclose SL, Weinstein B, Jones TS, Valleroy L, Fehrs L, Kassler WJ. Impact of increased legal access to needles and syringes on practices of
injecting drug users and police officers---Connecticut, 1992--1993.
J Acquir Immune Defic Syndr 1995;10:82--9.
Gershon RR. Infection control basis for recommending one-time use of sterile syringes and aseptic procedures for injection drug users.
J Acquir Immune Defic Syndr Hum Retrovirol 1998;18(suppl 1):S20--4.
Gleghorn AA, Doherty MC, Vlahov D, Celentano DD, Jones TS.
Inadequate bleach contact times during syringe cleaning among injection drug users. J Acquir Immune Defic Syndr 1994;7:767--72.
McCoy CB, Rivers JE, McCoy HV, et al. Compliance to bleach
disinfection protocols among injecting drug users in Miami. J Acquir Immune Defic Syndr 1994;7:773--6.
Fenton K, Peterman TA. HIV partner notification: taking a new look. AIDS 1997;11:1535--46.
CDC. HIV partner counseling and referral services. Guidance.
Atlanta, GA: US Department of Health and Human Services, CDC; 1998. Available
at www.cdc.gov/hiv/pubs/pcrs/pcrs-cov.htm.
CDC. Program Operations. Guidelines for STD Prevention. Partner Services. Atlanta, GA: US Department of Health and Human
Services, CDC. Updated June 28, 2001. Available at
www.cdc.gov/std/program/partners.pdf.
Cowan FM, French R, Johnson AM. The role and effectiveness of partner notification in STD control: a review. Genitourin Med 1996;72:247--52.
Kissinger PJ, Niccolai LM, Mangus M, et al. Partner notification for HIV and syphilis: effects on sexual behaviors and relationship stability.
Sex Transm Dis 2003; 30:75--82.
Hoxworth T, Spencer NE, Peterman TA, Craig T, Johnson S, Maher JE. Changes in partnerships and HIV risk behaviors after partner
notification. Sex Transm Dis 2003;30:83--8.
Rothenberg KH, Paskey SJ. The risk of domestic violence and women with HIV infection: implications for partner notification, public policy, and
the law. Am J Public Health 1995; 85:1569--76.
Maher JE, Peterson J, Hastings K, et al. Partner violence, partner notification, and women's decisions to have an HIV test. J Acquir Immune
Defic Syndr 2000;25:276--82.
Jones JL, Wykoff RF, Hollis SL, Longshore ST, Gamble WB, Jr. Gunn RA. Partner acceptance of health department notification of HIV
exposure, South Carolina. JAMA 1990;264:1284--6.
Wykoff RF, Heath CW Jr., Hollis SL, et al. Contact tracing to identify human immunodeficiency virus infection in a rural community.
JAMA 1988;259:3563--6.
Gostin LO, Webber DW. HIV infection and AIDS in the public health and health care systems: the role of law and litigation. JAMA
1998;279:1108--13.
Oxman AD, Scott EA, Sellors JW, et al. Partner notification for sexually transmitted diseases: an overview of the evidence. Can J Public
Health 1994;85(suppl 1):S41--7.
Macke BA, Maher JE. Partner notification in the United States: an evidence-based review. Am J Prev Med 1999;17:230--42.
Giesecke J, Ramstedt K, Granath F, Ripa T, Rado G, Westrell M.
Efficacy of partner notification for HIV infection. Lancet 1991;338:1096--100.
Members of the HIV Prevention in Clinical Care Working
Group
CDC: Sevgi Aral, Ph.D., Samuel W. Dooley, M.D., Mary L. Kamb, M.D., Jonathan
Kaplan, M.D., Mary Spink Neumann, Ph.D., Ida M. Onorato, M.D.,Thomas A.
Peterman, M.D., Kathryn J. Rauch, Renee Ridzon, M.D., J. Walton Senterfitt,
Ph.D., Atlanta, Georgia. Health Resources and Services Administration: Barbara
Aranda-Naranjo, Ph.D.; Michael Johnson, M.D., Rockville, Maryland. National Institutes of Health: Christopher M. Gordon, Ph.D.,
Rockville, Maryland. Infectious Diseases Society of America: John Bartlett, M.D., The
Johns Hopkins University School of Medicine, Baltimore, Maryland.
Consultants to the Working Group
Bruce D. Agins, M.D., New York State Department of Health
AIDS Institute, New York, New York; Kim W. Hamlett-Berry, Ph.D.,
Department of Veterans Affairs, Washington, D.C.; H. Hunter Handsfield,
M.D., University of Washington, Public Health-Seattle and King County,
Seattle, Washington; Fredrick Hecht, M.D., University of California, San
Francisco AIDS Program, San Francisco, California (HIVMA of IDSA); King K.
Holmes, M.D., University of Washington, Seattle, Washington; Kenneth
Mayer, M.D., Brown University School of Medicine, Providence, Rhode Island
(HIVMA of IDSA); Thomas C. Quinn, M.D., The Johns Hopkins University
School of Medicine, Baltimore, Maryland; Julie M. Scofield, National
Alliance of State and Territorial AIDS Directors, Washington, D.C.; Dan
Wohlfeiler, M.P.H., California Department of Public Health, Berkeley,
California. CDC Consultants: Joanna Buffington, Ph.D., James Buehler, M.D.,
Alan E. Greenberg, M.D., Kathleen Irwin, M.D., Harold W. Jaffe, M.D.,
Robert S. Janssen, M.D., Gary Marks, Ph.D., Allyn Nakashima, M.D., Esther
Sumartojo, Ph.D., Ronald O. Valdiserri, M.D., Jason Urbanowicz, J.D.,
Richard Wolitski, Ph.D., Kimberly Workowski, M.D., Centers for Disease
Control and Prevention, Atlanta, Georgia.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.