Prepared by
Scott A. Harper, M.D.1
Keiji Fukuda, M.D.1
Nancy J. Cox, Ph.D.1
Carolyn B. Bridges, M.D.2
1Division of Viral and Rickettsial Diseases
National Center for Infectious Diseases
2Epidemiology and Surveillance Division
National Immunization Program
The material is this report originated in the National Center for Infectious Diseases, James M. Hughes, M.D., Director, and the Division of Viral and Rickettsial Diseases, James LeDuc, Ph.D., Director; and the National Immunization Program, Walter A. Orenstein, M.D., Director, and Epidemiology and Surveillance Division, Melinda Wharton, M.D.,
Director.
Summary
This report summarizes recommendations by the Advisory Committee on Immunization Practices (ACIP) for
using intranasally administered, trivalent, cold-adapted, live, attenuated influenza vaccine (LAIV), which was approved for use
in the United States on June 17, 2003 (FluMist™, produced by MedImmune, Inc., Gaithersburg, Maryland). LAIV is
currently approved for use among healthy persons (i.e., those not at high risk for complications from influenza infection) aged
5--49 years. This report includes information regarding 1) vaccine composition and mechanisms of action; 2) comparison
between LAIV and trivalent inactivated influenza vaccine; 3) effectiveness and safety of LAIV; 4) transmission and stability of LAIV viruses; 5) recommendations and contraindications for using LAIV; and 6) dosage and administration of LAIV. This
report supplements the 2003 ACIP recommendations regarding prevention and control of influenza (CDC. Prevention and Control of Influenza: Recommendations of the Advisory Committee on Immunization Practices [ACIP]. MMWR 2003;52[No. RR-8]:1--36.)
Introduction
Each year, influenza virus infections cause substantial morbidity and mortality in the United States
(1). Prevention of influenza relies primarily on vaccination. Until recently, only inactivated influenza vaccine administered by injection
was available for use in the United States. Inactivated influenza vaccine is approved for persons aged
>6 months, both with and without chronic medical conditions. In 2003, an intranasal, trivalent, cold-adapted, live, attenuated vaccine (LAIV) was newly approved for use among healthy persons aged 5--49 years. LAIV adds an option for vaccinating healthy persons aged
5--49 years who either want to avoid influenza or who have close contact with persons at high risk for experiencing serious complications from influenza infection.
Description and Action Mechanisms of LAIV
LAIVs are in use in Russia and have been in development since the 1960s in the United States, where they have been evaluated as mono-, bi-, and trivalent formulations
(2--6). The newly licensed LAIV is produced by MedImmune,
Inc., (Gaithersburg, Maryland; http://www.medimmune.com) and marketed under the name FluMist™. It is a live, trivalent, intranasally administered vaccine that is
attenuated, producing mild or no signs or symptoms related to influenza virus infection;
temperature-sensitive, a property that limits the replication of the vaccine viruses at 38ºC--39ºC, and thus restricts
LAIV viruses from replicating efficiently in human lower airways; and
cold-adapted, replicating efficiently at
25ºC, a temperature that is permissive for replication of LAIV viruses,
but restrictive for replication of different wild-type viruses.
In animal studies, LAIV viruses replicate in the mucosa of the nasopharynx, inducing protective immunity
against viruses included in the vaccine, but replicate inefficiently in the lower airways or lungs. Identical to inactivated influenza vaccine, LAIV contains strains representative of each of the three influenza viruses recommended by the U.S. Public Health Service (1). For the 2003--04 influenza season, both inactivated influenza vaccine and LAIV contain A/New Caledonia/20/99-like (H1N1), A/Panama/2007/99-like (H3N2), and B/Hong Kong/330/2001-like viruses.
The first step in developing an LAIV was the derivation of two stably attenuated master donor viruses (MDV), one for
type A and one for type B influenza viruses. The two MDVs each acquired the cold-adapted, temperature-sensitive,
attenuated phenotypes through serial passage in viral culture conducted at progressively lower temperatures. The vaccine viruses in LAIV are reassortant viruses containing genes from these MDVs that confer attenuation, temperature sensitivity, and cold
adaptation and genes from the recommended contemporary wild-type influenza viruses, encoding the surface antigens
hemagglutinin (HA) and neuraminidase (NA). Thus, MDVs provide the stably attenuated vehicles for presenting influenza HA and NA antigens, to which the protective antibody response is directed, to the immune system. The reassortant vaccine viruses are grown in embryonated hens' eggs. After the vaccine is formulated and inserted into individual sprayers for
nasal administration, the vaccine must be stored at
--15ºC or colder.
The immunogenicity of the approved LAIV has been assessed in multiple studies
(7--15), which included approximately 100 children aged 5--17 years, and approximately 300 adults aged 18--49 years. LAIV virus strains replicate primarily in nasopharyngeal epithelial cells. The protective mechanisms induced by vaccination with LAIV are not completely
understood but appear to involve both serum and nasal secretory antibodies. No single laboratory measurement closely correlates
with protective immunity induced by LAIV.
Comparison of LAIV with Inactivated Influenza Vaccine
Major Similarities
LAIV and inactivated influenza vaccine contain strains of influenza viruses that are antigenically equivalent to the
annually recommended strains: one influenza A (H3N2) virus, one A (H1N1) virus, and one B virus. Each year, one or more
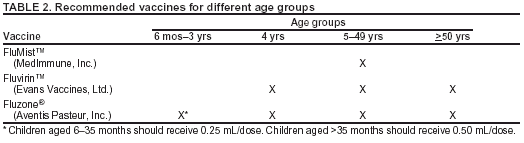
virus strains might be changed on the basis of global surveillance for influenza viruses and the emergence and spread of new strains. Viruses for both vaccines are grown in eggs. Both vaccines are administered annually to provide optimal protection against influenza infection. This report includes a more detailed comparison of LAIV with inactivated influenza vaccine (Tables 1 and
2).
Major Differences
Inactivated influenza vaccine contains killed viruses, whereas LAIV contains attenuated viruses still capable of
replication. LAIV is administered intranasally by sprayer, whereas inactivated influenza vaccine is administered intramuscularly by injection. LAIV is more expensive than inactivated influenza vaccine. LAIV is approved for use only among healthy
persons aged 5--49 years; inactivated influenza vaccine is approved for use among persons aged
>6 months, including those who are healthy and those with chronic medical conditions. This report includes a more detailed comparison of LAIV with inactivated influenza vaccine (Tables 1 and
2).
Efficacy and Effectiveness of LAIV
Efficacy Among Healthy Children
A randomized, double-blind, placebo-controlled trial among 1,602 healthy children initially aged 15--71 months
assessed the efficacy of the trivalent LAIV against culture-confirmed influenza during two seasons*
(8,9). This trial included subsets of 238 healthy children (163 vaccinees and 75 placebo recipients) aged 60--71 months who received two doses and 74 children
(54 vaccinees and 20 placebo recipients) aged 60--71 months who received a single dose during season one, and a subset
of 544 children (375 vaccinees and 169 placebo recipients) aged 60--84 months during season two. Children who
continued from season one to season two remained in the same study group. In season one, when vaccine and circulating virus
strains were well-matched, efficacy was 93% for all participants, regardless of age, among subjects receiving 2 doses of LAIV.
Efficacy was 87% in the 60--71-month subset for those who received 2 doses, and was 91% in the subset for those who received 1 or 2 doses. In season two, when the A (H3N2) component was not well-matched between vaccine and circulating virus
strains, efficacy was 86% overall and 87% among those aged 60--84 months. The vaccine was 92% efficacious in preventing culture-confirmed influenza during the two-season study. Other results included a 27% reduction in febrile otitis media and a
28% reduction in otitis media with concomitant antibiotic use. Receipt of LAIV also resulted in decreased fever and otitis
media among vaccine recipients who experienced influenza.
Effectiveness and Efficacy Among Healthy Adults
A randomized, double-blind, placebo-controlled trial among 4,561 healthy working adults aged 18--64 years
assessed multiple endpoints, including reductions in illness, absenteeism, health-care visits, and medication use during peak and total influenza outbreak periods (16). The study was conducted during the 1997--98 influenza season, when the vaccine
and circulating A (H3N2) strains were not well-matched. The study did not include laboratory virus testing of cases. During
peak outbreak periods, no difference was identified between LAIV and placebo recipients
experiencing any febrile episodes. However, vaccination was associated with reductions in severe febrile illnesses of 19% and febrile upper respiratory tract illnesses of 24%. Vaccination also was associated with fewer days of illness, fewer days of work lost, fewer days with
health-care provider visits, and reduced use of prescription antibiotics and over-the-counter medications.
Among the subset of 3,637 healthy adults aged 18--49 years, LAIV recipients (n = 2,411) had 26% fewer febrile
upper respiratory illness episodes; 27% fewer lost work days as a result of febrile upper respiratory illness; and 18%--37% fewer days of health-care provider visits caused by febrile illness, compared with placebo recipients (n = 1,226). Days of antibiotic use were reduced by 41%--45% in this age subset.
Another randomized, double-blind, placebo-controlled challenge study among 92 healthy adults (LAIV, n = 29; placebo,
n = 31; inactivated influenza vaccine, n = 32) aged 18--41 years assessed the efficacy of both LAIV and trivalent
inactivated vaccine (15). The overall efficacy of LAIV and inactivated influenza vaccine in preventing laboratory documented influenza from all three influenza strains combined was 85% and 71%, respectively, on the basis of experimental challenge by viruses to which study participants were susceptible before vaccination. The difference between the two vaccines was not
statistically significant.
Person-to-Person Transmission of Vaccine Viruses
Because LAIV contains live influenza viruses, a potential exists for transmission of these viruses from vaccinees to
other persons. Vaccinated immunocompetent children can shed vaccine viruses for
<3 weeks (6). One unpublished study in a
child care center setting assessed transmissibility of vaccine viruses from 98 vaccinated to 99 unvaccinated subjects, all aged 8--36 months. Eighty percent of vaccine recipients shed
>1 virus strain, with a mean of 7.6 days duration
(17). One influenza type B isolate was recovered from a placebo recipient and was confirmed to be vaccine-type virus. The estimated probability of acquiring vaccine virus after close contact with a single LAIV recipient was 0.58%--2.4%. The type B isolate retained the cold-adapted, temperature-sensitive, attenuated phenotype, and it possessed the same genetic sequence as a virus shed from a
vaccine recipient in the same children's play group.
Stability of Vaccine Viruses
In clinical trials, viruses shed by vaccine recipients have been phenotypically stable. In one study, nasal and throat
swab specimens were collected from 17 study participants for 2 weeks after vaccine receipt
(18). Virus isolates were analyzed by multiple genetic techniques. All isolates retained the LAIV genotype after replication in the human host, and all retained the cold-adapted and temperature-sensitive phenotypes.
Recommendations for Influenza Vaccination
Recommendations for inactivated influenza vaccination have targeted specific groups for annual immunization,
including persons aged >6 months who are at high risk for complications from influenza because of age or presence of certain
medical conditions, persons who are in close contact with those at high risk, persons aged 50--64 years, and close contacts of
infants aged 0--6 months (1). Vaccination with inactivated influenza vaccine is also encouraged when feasible for children aged 6--23 months and their close contacts and caregivers. In addition, physicians should administer inactivated influenza vaccine to
any person who wishes to reduce the likelihood of becoming ill with influenza. Recommendations for use of inactivated
influenza vaccine are located at
http://www.cdc.gov/mmwr/PDF/rr/rr5208.pdf.
Recommendations for Using Live, Attenuated Influenza Vaccine
LAIV is an option for vaccination of healthy persons aged 5--49 years, including persons in close contact with groups
at high risk and those wanting to avoid influenza (Tables 1 and 2). Possible advantages of LAIV include its potential to induce a broad mucosal and systemic immune response, its ease of administration, and the acceptability of an intranasal rather
than intramuscular route of administration
(1).
Persons Who Should Not Be Vaccinated with LAIV
The following populations should not be vaccinated with LAIV:
persons aged <5 years or those aged
>50 years;†
persons with asthma, reactive airways disease or other chronic disorders of the pulmonary or cardiovascular
systems; persons with other underlying medical conditions, including such metabolic diseases as diabetes, renal dysfunction, and hemoglobinopathies; or persons with known or suspected immunodeficiency diseases or who are
receiving immunosuppressive therapies;†
children or adolescents receiving aspirin or other salicylates (because of the association of Reye syndrome with
wild-type influenza infection);†
persons with a history of Guillain-Barré syndrome;
pregnant women;† or
persons with a history of hypersensitivity, including anaphylaxis, to any of the components of LAIV or to eggs.
Close Contacts of Persons at High Risk for Complications from Influenza
Close contacts of persons at high risk for complications from influenza should receive influenza vaccine to
reduce transmission of wild-type influenza viruses to persons at high risk. No data are available assessing the risk for transmission of LAIV from vaccine recipients to immunosuppressed contacts. In the absence of such data, use of inactivated influenza
vaccine is preferred for vaccinating household members, health-care workers, and others who have close contact
with immunosuppressed persons because of the theoretical risk that a live, attenuated vaccine virus could be transmitted to
the immunosuppressed person and cause disease. Otherwise, no preference is given to either inactivated influenza vaccine or LAIV for vaccination of healthy persons aged 5--49 years in close contact with all other groups at high risk.
Timing of LAIV Administration
Administration of LAIV is not subject to tiered timing recommendations because it is not approved for use
among populations at high risk. The optimal time to vaccinate is usually in October and November, but providers can
begin vaccinating with LAIV as soon as vaccine supplies are available. Children aged 5--8 years who have never received influenza vaccine should receive LAIV for the first time in October or earlier because they need a second dose 6--10 weeks after the initial dose.
Dosage, Administration, and Storage
LAIV Dosage
LAIV is intended for intranasal administration only and should not be administered by the intramuscular, intradermal,
or intravenous route. LAIV must be stored at
--15ºC or colder. LAIV should not be stored in a frost-free freezer (because
the temperature might cycle above
--15ºC), unless a manufacturer-supplied freezer box is used. LAIV must be thawed
before administration. This can be accomplished by holding an individual sprayer in the palm of the hand until thawed,
with subsequent immediate administration. Alternatively, the vaccine can be thawed in a refrigerator and stored at 2ºC--8ºC for
<24 hours before use. Vaccine should not be refrozen after thawing. LAIV is supplied in a prefilled single-use
sprayer containing 0.5 mL of vaccine. Approximately 0.25 mL (i.e., half of the total sprayer contents) is sprayed into the first nostril while the recipient is in the upright position. An attached dose-divider clip is removed from the sprayer to administer the second half of the dose into the other nostril. If the vaccine recipient sneezes after administration, the dose should not be repeated.
LAIV should be administered annually according to the following schedule:
• Children aged 5--8 years previously unvaccinated at any time with either LAIV or inactivated influenza vaccine
should receive 2 doses§ of LAIV separated by 6--10 weeks.
• Children aged 5--8 years previously vaccinated at any time
with either LAIV or inactivated influenza vaccine should
receive 1 dose of LAIV. They do not require a second dose.
• Persons aged 9--49 years should receive 1 dose of LAIV.
LAIV can be administered to persons with minor acute illnesses (e.g., diarrhea or mild upper respiratory tract infection with or without fever). However, if clinical judgment indicates nasal congestion is present that might impede delivery
of the vaccine to the nasopharyngeal mucosa, deferral of administration should be considered until resolution of the illness.
Whether concurrent administration of LAIV with other vaccines affects the safety or efficacy of either LAIV or
the simultaneously administered vaccine is unknown. In the absence of specific data indicating interference, following the ACIP general recommendations for immunization is prudent
(19). Inactivated vaccines do not interfere with the immune
response to other inactivated vaccines or to live vaccines. An inactivated vaccine can be administered either simultaneously or at any time before or after LAIV. Two live vaccines not administered on the same day should be administered
>4 weeks apart when possible.
LAIV Administration and Use of Influenza Antiviral Medications
The effect on safety and efficacy of LAIV coadministration with influenza antiviral medications has not been
studied. However, because influenza antivirals reduce replication of influenza viruses, LAIV should not be administered until 48 hours after cessation of influenza antiviral therapy, and influenza antiviral medications should not be administered for 2 weeks after receipt of LAIV.
LAIV Storage
LAIV must be stored at --15ºC or colder. LAIV should not be stored in a frost-free freezer because the temperature
might cycle above --15ºC, unless a manufacturer-supplied freezer box or other strategy is used. LAIV may be thawed in a refrigerator and stored at
2ºC--8ºC for
<24 hours before use. It should not be refrozen after thawing. Additional information is available
at Wyeth Product Quality (1-800-411-0086) or at http://www.FluMist.com.
Side Effects and Adverse Reactions
Twenty prelicensure clinical trials assessed the safety of the approved LAIV. In these combined studies,
approximately 28,000 doses of the vaccine were administered to >20,000 subjects. A subset of these trials were randomized, placebo-controlled studies in which >4,000 healthy children aged 5--17 years and >2,000 healthy adults aged 18--49 years were
vaccinated. The incidence of adverse events possibly complicating influenza (e.g., pneumonia, bronchitis, bronchiolitis,
or central nervous system events) was not statistically different among LAIV and placebo recipients aged 5--49 years.
Children
Signs and symptoms reported more often among vaccine recipients than placebo recipients included runny nose or nasal congestion (20%--75%), headache (2%--46%), fever (0%--26%), and vomiting (3%--13%), abdominal pain (2%),
and myalgias (0%--21%) (7,12,14,20--22). These symptoms were associated more often with the first dose and were self-limited. In a subset of healthy children aged 60--71 months from one clinical trial
(8,9), certain signs and symptoms were
reported more often among LAIV recipients after the first dose (n = 214) than placebo recipients (n = 95) (e.g., runny nose, 48.1% versus 44.2%; headache, 17.8% versus 11.6%; vomiting, 4.7% versus 3.2%; myalgias, 6.1% versus 4.2%), but
these differences were not statistically significant. Unpublished data from a study including subjects aged 1--17 years indicated an increase in asthma or reactive airways disease in the subset aged 12--59 months. Because of this, LAIV is not approved for
use among children aged <60 months (see Recommendations for Using Live, Attenuated Influenza Vaccine).
Adults
Among adults, runny nose or nasal congestion (28%--78%), headache (16%--44%), and sore throat (15%--27%) have
been reported more often among vaccine recipients than placebo recipients
(16,23,24). In one clinical trial
(16), among a subset of healthy adults aged 18--49 years, signs and symptoms reported more frequently among LAIV recipients (n = 2,548) than placebo recipients (n = 1,290) within 7 days after each dose included cough (13.9% versus 10.8%); runny nose (44.5%
versus 27.1%); sore throat (27.8% versus 17.1%); chills (8.6% versus 6.0%); and tiredness/weakness (25.7% versus 21.6%).
Safety Among Groups at High Risk from Influenza-Related Morbidity
Until additional data are acquired, persons at high risk for experiencing complications from influenza infection (e.g., immunocompromised patients; patients with asthma, cystic fibrosis, or chronic obstructive pulmonary disease; or
persons aged >65 years) should not be vaccinated with LAIV. Protection from influenza in these groups should be accomplished by using inactivated influenza vaccine (see Recommendations for Using Live, Attenuated Influenza Vaccine).
Serious Adverse Events
Serious adverse events among healthy children aged 5--17 years or healthy adults aged 18--49 years occurred at a rate
of <1%. Surveillance should continue for adverse events that might not have been detected in previous studies.
Kendal AP, Maassab HF, Alexandrova GI, Ghendon YZ. Development of cold-adapted recombinant live, attenuated influenza A vaccines in
the U.S.A. and U.S.S.R. Antiviral Res 1981;1:339--65.
Maassab HF, DeBorde DC. Development and characterization of cold-adapted viruses for use as live virus vaccines. Vaccine 1985;3:355--69.
Murphy BR. Use of live attenuated cold-adapted influenza A reassortant virus vaccines in infants, children, young adults, and elderly adults.
Infect Dis Clin Pract 1993;2:174--81.
Potter CW. Attenuated influenza virus vaccines. Rev Med Virol 1994;4:279--92.
Clements ML, Stephens I. New and improved vaccines against influenza. In: Levine MM, Woodrow GC, Kasper JB, et al., eds. New
generation vaccines. New York: Marcel Dekker, Inc 1997:645--70.
King JC, Lagos R, Bernstein DI, et al. Safety and immunogenicity of low and high doses of trivalent live cold-adapted influenza
vaccine administered intranasally as drops or spray to healthy children. J Infect Dis 1998;177:1394--7.
Belshe RB, Mendelman PM, Treanor J, et al. Efficacy of live attenuated, cold-adapted, trivalent, intranasal influenzavirus vaccine in children. N
Engl J Med 1998;338:1405--12.
Belshe RB, Gruber WC, Mendelman PM, et al. Efficacy of vaccination with live attenuated, cold-adapted, trivalent, intranasal influenza
virus vaccine against a variant (A/Sydney) not contained in the vaccine. J Peds 2000;136:168--75.
Belshe RB, Gruber WC, Mendelman PM, et al. Correlates of immune protection induced by live, attenuated, cold-adapted, trivalent,
intranasal influenza virus vaccine. J Infect Dis 2000;181:1133--7.
Boyce TG, Gruber WC, Coleman-Dockery SD, et al. Mucosal immune response to trivalent live attenuated intranasal influenza vaccine in
children. Vaccine 2000;18:82--8.
Zangwill KM, Droge J, Mendelman P, et al. Prospective, randomized, placebo-controlled evaluation of the safety and immunogenicity of three
lots of intranasal trivalent influenza vaccine among young children. Pediatr Infect Dis J 2001;20:740--6.
Bernstein DI, Yan L, Treanor J, et al. Effect of yearly vaccinations with live, attenuated, cold-adapted, trivalent, intranasal influenza vaccines
on antibody responses in children. Pediatr Infect Dis J
2003;22:28--34.
Nolan T, Lee M-S, Cordova JM, et al. Safety and immunogenicity of a live-attenuated influenza vaccine blended and filled at two
manufacturing facilities. Vaccine 2003;21:1224--31.
Treanor JJ, Kotloff K, Betts RF, et al. Evaluation of trivalent, live, cold-adapted (CAIV-T) and inactivated (TIV) influenza vaccines in prevention
of virus infection and illness following challenge of adults with wild-type influenza A (H1N1), A (H3N2), and B viruses. Vaccine 2000;18:899--906.
Nichol KL, Mendelman PM, Mallon KP, et al. Effectiveness of live, attenuated intranasal influenza virus vaccine in healthy, working adults:
a randomized controlled trial. JAMA 1999;281:137--144.
Vesikari T, et al. Randomized, double-blind, placebo-controlled trial of the safety, transmissibility and phenotypic stability of a live, attenuated,
cold-adapted influenza virus vaccine (CAIV-T) in children attending day care [Abstract G-450]. Presented at the 41st Annual Interscience Conference
on Antimicrobial Agents and Chemotherapy (ICAAC), Chicago, IL, 2001.
Cha TA, Kao K, Zhao J, Fast PE, Mendelman PM, Arvin A. Genotypic stability of cold-adapted influenza virus vaccine in an efficacy clinical trial.
J Clin Micro 2000;38:839--45.
King JC, Fast PE, Zangwill KM, et al. Safety, vaccine virus shedding and immunogenicity of trivalent, cold-adapted, live attenuated
influenza vaccine administered to human immunodeficiency virus-infected and noninfected children. Pediatr Infect Dis J 2001;20:1124--31.
Redding G, Walker RE, Hessel C, et al. Safety and tolerability of cold-adapted influenza virus vaccine in children and adolescents with
asthma. Pediatr Infect Dis J 2002;21:44--8.
Piedra PA, Yan L, Kotloff K, et al. Safety of the trivalent, cold-adapted influenza vaccine in preschool-aged children. Pediatrics 2002;110:662--72.
Jackson LA, Holmes SJ, Mendelman PM, Huggins L, Cho I, Rhorer J. Safety of a trivalent live attenuated intranasal influenza vaccine,
FluMist™, administered in addition to parenteral trivalent inactivated influenza vaccine to seniors with chronic medical conditions. Vaccine 1999;17:1905--9.
King JC, Treanor J, Fast PE, et al. Comparison of the safety, vaccine virus shedding and immunogenicity of influenza virus vaccine, trivalent, types
A and B, live cold-adapted, administered to human immunodeficiency virus (HIV)-infected and non-HIV-infected adults. J Infect Dis
2000;181:725--8.
* Influenza seasons usually occur October---May.
† These persons should receive inactivated influenza vaccine.
§ One dose equals 0.5 mL, divided equally between each nostril.
Advisory Committee on Immunization Practices Membership List, May 2003
Chairman: John F. Modlin, M.D., Professor of Pediatrics and Medicine, Dartmouth Medical School, Lebanon, New Hampshire.
Executive Secretary: Dixie E. Snider, Jr., M.D., Associate Director for Science, Centers for Disease Control and Prevention, Atlanta, Georgia.
Members: Guthrie S. Birkhead, M.D., New York State Department of Health, Albany, New York; Dennis A. Brooks, M.D., Johnson Medical
Center, Baltimore, Maryland; Judith Campbell, M.D., Baylor College of Medicine, Houston, Texas; Jaime Deseda-Tous, M.D., San Jorge Children's Hospital, San Juan, Puerto Rico; Reginald Finger, M.D., Focus on the Family, Colorado Springs, Colorado; Janet R. Gilsdorf, M.D., University of Michigan, Ann Arbor, Michigan; Celine I. Hanson, M.D., Texas Department of Health, Houston, Texas; Myron J. Levin, M.D., University of Colorado School of
Medicine, Denver, Colorado; Gregory A. Poland, M.D., Mayo Clinic and Foundation, Rochester, Minnesota; John B. Salamone, NIAF, Washington, D.C.; Lucy S. Tompkins, M.D., Ph.D., Stanford University Medical Center, Stanford, California; and Richard Zimmerman, M.D., University of Pittsburgh School
of Medicine, Pittsburgh, Pennsylvania.
Ex-Officio Members: James E. Cheek, M.D., Indian Health Service, Albuquerque, New Mexico; Col. Benedict M. Diniega, M.D., Department
of Defense, Falls Church, Virginia; Geoffrey S. Evans, M.D., Health Resources and Services Administration, Rockville, Maryland; Bruce Gellin, M.D., National Vaccine Program Office, Washington, D.C.; T. Randolph Graydon, Centers for Medicare and Medicaid Services, Baltimore, Maryland; Carole Heilman, Ph.D., National Institutes of Health, Bethesda, Maryland; Karen Midthun, M.D., Food and Drug Administration, Bethesda, Maryland; and Kristin Lee Nichol, M.D., Veterans Administration Medical Center, Minneapolis, Minnesota.
Liaison Representatives: American Academy of Family Physicians, Richard D. Clover, M.D., Louisville, Kentucky, and Martin Mahoney, M.D., Ph.D., Clarence, New York; American Academy of Pediatrics, Jon Abramson, M.D., Winston-Salem, North Carolina, and Carol Baker, M.D., Houston,
Texas; American Association of Health Plans, Robert Scallettar, M.D., North Haven, Connecticut; American Collage Health Association, James C. Turner, M.D., Charlottesville, Virginia; American College of Obstetricians and Gynecologists, Stanley Gall, M.D., Louisville, Kentucky; American College of Physicians, Kathleen M. Neuzil, M.D., Seattle, Washington; American Medical Association, Litjen Tan, Ph.D., Chicago, Illinois; American Pharmaceutical Association, Stephan L. Foster, Pharm.D., Memphis, Tennessee; Association of Teachers of Preventive Medicine, W. Paul McKinney, M.D., Louisville, Kentucky; Canadian National Advisory Committee on Immunization, Monica Naus, M.D., Vancouver, British Columbia, Canada; Healthcare
Infection Control Practices Advisory Committee, Jane D. Siegel, M.D., Dallas, Texas; Infectious Diseases Society of America, Samuel L. Katz, M.D., Durham, North Carolina, and William Schaffner, M.D., Nashville, Tennessee; London Department of Health, David M. Salisbury, M.D., London, United
Kingdom; National Association of County and City Health Officials, J. Henry Hershey, M.D., Christiansburg, Virginia; National Coalition for Adult Immunization, David A. Neumann, Ph.D., Bethesda, Maryland; National Immunization Council and Child Health Program, Mexico, Jose Ignacio Santos, M.D., Mexico
City, Mexico; National Medical Association, Rudolph E. Jackson, M.D., Atlanta, Georgia; National Vaccine Advisory Committee, Georges Peter,
M.D., Providence, Rhode Island; and Pharmaceutical Research and Manufacturers of America, Geno Germano, St. Davids, Pennsylvania, and Geno Germano,
St. Davids, Pennsylvania.
ACIP Influenza Working Group
Chair: Richard Zimmerman, M.D., Pittsburgh, Pennsylvania.
Members: Kristin Lee Nichol, M.D., and Margaret B. Rennels, M.D., ACIP; Jon Abramson, M.D., American Academy of Pediatrics; Stanley A.
Gall, M.D., American College of Obstetricians and Gynecologists; Linda C. Lambert, Ph.D., National Institutes of Health; Roland A. Levandowski, M.D.,
and ChrisAnna M. Mink, M.D., Food and Drug Administration; Kathleen M. Neuzil, M.D., American College of Physicians; Fred Ruben,
M.D., Pharmaceutical Research and Manufacturers of America; William Schaffner, M.D., Infectious Diseases Society of America; Richard D. Clover, M.D.,
and Martin Mahoney, M.D., Ph.D., American Academy of Family Physicians; and Nancy J. Cox, Ph.D., Keiji Fukuda, M.D., Carolyn B. Bridges,
M.D., Dennis J. O'Mara, and William W. Thompson, Ph.D., Centers for Disease Control and Prevention.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.