Updated U.S. Public Health Service Guidelines for the
Management of Occupational Exposures to HIV and Recommendations
for Postexposure Prophylaxis
Please note: An update has been published for this report. To view the update, please click here.
Prepared by
Adelisa L. Panlilio, MD1
Denise M. Cardo, MD1
Lisa A. Grohskopf, MD2
Walid Heneine, PhD2
Clara Sue Ross, MD3
1Division of Healthcare Quality Promotion, National Center for Infectious Diseases
2Division of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention
3Division of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health
The material in this report originated in the National Center for Infectious Diseases, Anne Schuchat, MD, Acting Director; Division of Healthcare
Quality Promotion, Denise M. Cardo, MD, Director.
Corresponding preparer: Adelisa L. Panlilio, MD, MPH, Division of Healthcare Quality Promotion, National Center for Infectious Diseases, CDC,
1600 Clifton Rd., NE, MS E-68, Atlanta, GA 30333. Telephone: 404-498-1265; Fax: 404-498-1244; E-mail:
alp4@cdc.gov.
Summary
This report updates U.S. Public Health Service recommendations for the management of health-care personnel (HCP)
who have occupational exposure to blood and other body fluids that might contain human immunodeficiency virus
(HIV). Although the principles of exposure management remain unchanged, recommended HIV postexposure prophylaxis
(PEP) regimens have been changed. This report emphasizes adherence to HIV PEP when it is indicated for an exposure,
expert consultation in management of exposures, follow-up of exposed workers to improve adherence to PEP, and monitoring
for adverse events, including seroconversion. To ensure timely postexposure management and administration of HIV
PEP, clinicians should consider occupational exposures as urgent medical concerns.
Introduction
Although preventing exposures to blood and body fluids is the primary means of preventing occupationally acquired
human immunodeficiency virus (HIV) infection, appropriate postexposure management is an important element of workplace
safety. In 1996, the first U.S. Public Health Service (PHS) recommendations for the use of postexposure prophylaxis (PEP)
after occupational exposure to HIV were published; these recommendations have been updated twice
(1--3). Since publication of the most recent guidelines in 2001, new antiretroviral agents have been approved by the Food and Drug
Administration (FDA), and additional information has
become available regarding the use and safety of HIV PEP. In August 2003,
CDC convened a meeting of a PHS interagency working group* and consultants to assess use of HIV PEP. On the basis of
this discussion, the PHS working group decided that updated recommendations for the management of occupational exposure
to HIV were warranted.
This report modifies and expands the list of antiretroviral medications that can be considered for use as PEP. This report
also emphasizes prompt management of occupational exposures, selection of tolerable regimens, attention to potential
drug interactions involving drugs that could be included in HIV PEP regimens and other medications, consultation with
experts for postexposure management strategies (especially determining whether an exposure has actually occurred) and selection
of HIV PEP regimens, use of HIV rapid testing, and counseling and follow-up of exposed personnel.
Recommendations on the management of occupational
exposures to hepatitis B virus or hepatitis C virus have
been published previously (3) and are not included in this report. Recommendations for nonoccupational (e.g., sexual,
pediatric, and perinatal) HIV exposures also have been published previously
(4--6).
Definition of Health-Care Personnel and Exposure
The definitions of health-care personnel (HCP) and occupational exposures are unchanged from those used in 2001
(3). The term HCP refers to all paid and unpaid persons working in health-care settings who have the potential for exposure
to infectious materials (e.g., blood, tissue, and specific body fluids and medical supplies, equipment, or environmental
surfaces contaminated with these substances). HCP might include, but are not limited to, emergency medical service personnel,
dental personnel, laboratory personnel, autopsy personnel, nurses, nursing assistants, physicians, technicians, therapists,
pharmacists, students and trainees, contractual staff not employed by the health-care facility, and persons not
directly involved in patient care but potentially exposed to blood and body fluids (e.g., clerical, dietary, housekeeping, maintenance, and
volunteer personnel). The same principles of exposure management could be applied to other workers who have potential
for occupational exposure to blood and body fluids in other settings.
An exposure that might place HCP at risk for HIV infection is defined as a percutaneous injury (e.g., a needlestick or
cut with a sharp object) or contact of mucous membrane or nonintact skin (e.g., exposed skin that is chapped, abraded,
or afflicted with dermatitis) with blood, tissue, or other body fluids that are potentially infectious. In addition to blood
and visibly bloody body fluids, semen and vaginal secretions also are considered potentially infectious. Although semen and
vaginal secretions have been implicated in the sexual transmission of HIV, they have not been implicated in occupational
transmission from patients to HCP. The following fluids also are considered potentially infectious: cerebrospinal fluid, synovial
fluid, pleural fluid, peritoneal fluid, pericardial fluid, and amniotic fluid. The risk for transmission of HIV infection from
these fluids is unknown; the potential risk to HCP from occupational exposures has not been assessed by epidemiologic studies
in health-care settings. Feces, nasal secretions, saliva, sputum, sweat, tears, urine, and vomitus are not considered
potentially infectious unless they are visibly bloody; the risk for transmission of HIV infection from these fluids and materials is low
(7).
Any direct contact (i.e., contact without barrier protection) to concentrated virus in a research laboratory or
production facility requires clinical evaluation. For human bites, clinical evaluation must include the possibility that both the
person bitten and the person who inflicted the bite were exposed to bloodborne pathogens. Transmission of HIV infection by
this route has been reported rarely, but not after an occupational exposure
(8--12).
Risk for Occupational Transmission of HIV
The risks for occupational transmission of HIV have been described; risks vary with the type and severity of
exposure (2,3,7). In prospective studies of HCP, the average risk for HIV transmission after a percutaneous exposure to
HIV-infected blood has been estimated to be approximately 0.3% (95% confidence interval [CI] = 0.2%--0.5%)
(7) and after a mucous membrane exposure, approximately 0.09%
(CI = 0.006%--0.5%) (3). Although episodes of HIV transmission
after nonintact skin exposure have been documented, the average risk for transmission by this route has not been
precisely quantified but is estimated to be less than the risk for mucous membrane exposures. The risk for transmission after
exposure to fluids or tissues other than HIV-infected blood also has not been quantified but is probably considerably lower than
for blood exposures.
Epidemiologic and laboratory studies suggest that multiple factors might affect the risk for HIV transmission after
an occupational exposure (3). In a retrospective case-control study of HCP who had percutaneous exposure to HIV,
increased risk for HIV infection was associated with exposure to a larger quantity of blood from the source person as indicated by 1)
a device (e.g., a needle) visibly contaminated with the patient's blood, 2) a procedure that involved a needle being
placed directly in a vein or artery, or 3) a deep injury. The risk also was increased for exposure to blood from source persons
with terminal illness, possibly reflecting either the higher titer of HIV in blood late in the course of acquired
immunodeficiency syndrome (AIDS) or other factors (e.g., the presence of syncytia-inducing strains of HIV). A laboratory study
that demonstrated that more blood is transferred by deeper injuries and hollow-bore needles lends further support for the
observed variation in risk related to blood quantity
(3).
The use of source-person viral load as a surrogate measure of viral titer for assessing transmission risk has not yet
been established. Plasma viral load (e.g., HIV RNA) reflects only the level of cell-free virus in the peripheral blood;
latently infected cells might transmit infection in the absence of viremia. Although a lower viral load (e.g., <1,500 RNA copies/mL)
or one that is below the limits of detection probably
indicates a lower titer exposure, it does not rule out the possibility
of transmission.
Antiretroviral Agents for PEP
Antiretroviral agents from five classes of drugs are currently available to treat HIV infection
(13,14). These include the nucleoside reverse transcriptase inhibitors (NRTIs), nucleotide reverse transcriptase inhibitors (NtRTIs), nonnucleoside
reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs), and a single fusion inhibitor. Only antiretroviral agents
approved by FDA for treatment of HIV infection are included in these guidelines. The recommendations in this report
provide guidance for two- or-more drug PEP regimens on the basis of the level of risk for HIV transmission represented by
the exposure (Tables 1 and 2;
Appendix).
Toxicity and Drug Interactions of Antiretroviral Agents
Persons receiving PEP should complete a full 4-week regimen
(3). However, as a result of toxicity and side effects
among HCP, a substantial proportion of HCP have been unable to complete a full 4-week course of HIV PEP
(15--20). Because all antiretroviral agents have been associated with side effects (Table 3), the toxicity profile of these agents, including
the frequency, severity, duration, and reversibility of side effects, is an important consideration in selection of an HIV
PEP regimen. The majority of data concerning adverse events have been reported primarily for persons with established
HIV infection receiving prolonged antiretroviral therapy and therefore might not reflect the experience of uninfected persons
who take PEP. Anecdotal evidence from clinicians knowledgeable about HIV treatment indicates that antiretroviral agents
are tolerated more poorly among HCP taking HIV PEP than among HIV-infected patients on antiretroviral medications.
Side effects have been reported frequently by persons taking antiretroviral agents as PEP
(15--23). In multiple instances, a substantial (range: 17%--47%) proportion of HCP taking PEP after occupational exposures to HIV-positive sources did
not complete a full 4-weekcourse of therapy because of inability to tolerate the drugs
(15--17,19,20). Data from the National Surveillance System for Health Care Workers (NaSH), CDC's occupational surveillance system for occupational exposures
and infections in hospitals, for June 1995--December 2004 indicate that 401 (46.9%) of 921 HCP with at least one
follow-up visit after starting PEP experienced one or more symptoms. The symptom reported most frequently was nausea
(26.5%), followed by malaise and fatigue (22.8%) (CDC, unpublished data, 2005). Of 503 HCP who stopped HIV PEP
prematurely (<28 days), 361 (24.0%) did so because
of adverse effects of the drugs. Similar data have been reported from the
Italian Registry of Antiretroviral Postexposure Prophylaxis, which includes data primarily on HCP taking PEP but also collects
data on those taking PEP after nonoccupational exposures
(18). In multivariate analysis, those taking regimens that include PI
were more likely to experience PEP-associated side effects and to discontinue PEP prematurely (<28 days). Because side effects
are frequent and particularly because they are cited as a major reason for not completing PEP regimens as prescribed, the
selection of regimens should be heavily influenced toward those that are tolerable for short-term use.
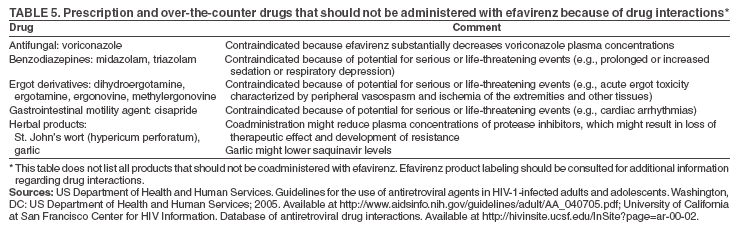
In addition, all approved antiretroviral agents might have potentially serious drug interactions when used with certain
other drugs, requiring careful evaluation of concomitant medications, including over-the-counter medications and
supplements (e.g., herbals), used by an exposed person before prescribing PEP and close monitoring for toxicity of anyone receiving
these drugs (24--33) (Tables 3--5). PIs and NNRTIs have the greatest potential for interactions with other drugs.
Information regarding potential drug interactions has been published
(13,24--33). Additional information is included in
the manufacturers' package inserts. Because of interactions, certain drugs should not be administered concomitantly with PIs
or with efavirenz (EFV) (Tables 4 and 5). Consultation with a pharmacist might be considered.
Selection of HIV PEP Regimens
Determining which agents and how many to use or when to alter a PEP regimen is primarily empiric
(34). Guidelines for treating HIV infection, a condition typically involving a high total body burden of HIV, recommend use of three or
more drugs (13,14); however, the applicability of these recommendations to PEP is unknown. Among HIV-infected
patients, combination regimens with three or more antiretroviral agents have proved superior to monotherapy and
dual-therapy regimens in reducing HIV viral load, reducing incidence of opportunistic infections and death, and delaying onset of
drug resistance (13,14). In theory, a combination of drugs with activity at different stages in the viral replication cycle
(e.g., nucleoside analogues with a PI) might offer an additive preventive effect in PEP, particularly for occupational exposures
that pose an increased risk for transmission or for transmission of a resistant virus. Although use of a three- (or more) drug
regimen might be justified for exposures that pose an increased risk for transmission, whether the potential added toxicity of a third
or fourth drug is justified for lower-risk exposures is uncertain, especially in the absence of data supporting increased efficacy
of
more drugs in the context of occupational PEP. Offering a two-drug regimen is a viable option, primarily because the
benefit of completing a full course of this regimen exceeds the benefit of adding the third agent and risking noncompletion
(35). In addition, the total body burden of HIV is substantially lower among exposed HCP than among persons with established
HIV infection. For these reasons, the recommendations in this report provide guidance for two- and three- (or more) drug
PEP regimens on the basis of the level of risk for HIV transmission represented by the exposure (Tables 1 and
2; Appendix).
Resistance to Antiretroviral Agents
Known or suspected resistance of the source virus to antiretroviral agents, particularly those that might be included in a
PEP regimen, is a concern for persons making decisions about PEP
(36). Drug resistance to all available antiretroviral agents
has been reported, and cross-resistance within drug classes is frequent
(37). Although occupational transmission of
drug-resistant HIV strains has been reported despite PEP with combination drug regimens
(36,38--40), the effect of exposure to a
resistant virus on transmission and transmissibility is not well understood.
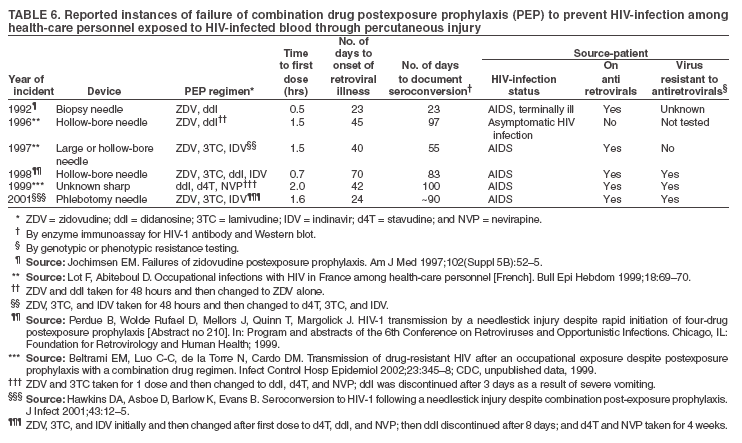
Since publication of the previous guidelines, an additional report of an occupational HIV seroconversion
despite combination HIV PEP has been published (Table 6)
(38), bringing the total number of reports worldwide to six.
The exposure was a percutaneous injury sustained by a nurse performing a phlebotomy on a heavily treatment-experienced
patient. At the time of the exposure, the source patient was failing treatment with stavudine (d4T), lamivudine (3TC),
ritonavir (RTV), and saquinavir (SQV) and had a history of previous treatment with zidovudine (ZDV) and zalcitabine
(ddC). Genotypic resistance testing performed within 1 month of the exposure suggested resistance to ZDV and 3TC.
Phenotypic testing confirmed resistance to 3TC but demonstrated relative susceptibility to ZDV and d4T. The source virus
demonstrated no evidence of resistance to nevirapine (NVP) or other NNRTIs. The initial HIV PEP regimen started within 95 minutes
of the exposure was ZDV, 3TC, and indinavir. The worker was referred to a hospital where the regimen was changed within
6 hours of the exposure to didanosine (ddI), d4T, and NVP because of concerns regarding possible drug resistance to certain
or all of the components of the initial PEP regimen. The exposed worker stopped ddI
after 8 days because of symptoms but continued to take d4T and NVP, stopping at day 24 because of a generalized macular pruritic rash and
mild thrombocytopenia. Seroconversion was documented at 3 months. Sequencing of viruses from the source and exposed
worker demonstrated their close relatedness. Virus
from the worker demonstrated the same resistance patterns as those in the
source patient. In addition, the worker's virus had a mutation suggesting resistance to the NNRTI class
(38).
Empiric decisions regarding the presence of antiretroviral drug resistance are often difficult because patients frequently
take more than one antiretroviral agent. Resistance should be suspected in a source patient when clinical progression of disease or
a persistently increasing viral load or decline in CD4+ T-cell count occurs despite therapy, or when no virologic
response to therapy occurs. However, resistance testing of the source virus at the time of an exposure is impractical because the results
will not be available in time to influence the choice of the initial PEP regimen. No data suggest that modification of a
PEP regimen after resistance testing results become available (usually 1--2 weeks) improves efficacy of PEP
(41).
Antiretroviral Drugs During Pregnancy
Data regarding the potential effects of antiretroviral drugs on the developing fetus or neonate are limited
(3). Carcinogenicity and mutagenicity are evident in certain in vitro screening tests for ZDV and all other FDA-licensed
NRTIs. The relevance of animal data to humans is unknown; however, because teratogenic effects were reported among primates
at drug exposures similar to those representing human therapeutic exposure, pregnant women should not use efavirenz
(EFV). Indinavir (IDV) is associated with infrequent side
effects in adults (i.e., hyperbilirubinemia and renal stones) that could
be problematic for a newborn. Because the half-life of IDV in adults is short, these concerns might be relevant only if the drug
is administered shortly before delivery. Other concerns regarding use of PEP during pregnancy have been raised by reports
of mitochondrial dysfunction leading to neurologic disease and death among uninfected children whose mothers had
taken antiretroviral drugs to prevent perinatal HIV transmission and of fatal and nonfatal lactic acidosis in pregnant women
treated throughout gestation with a combination of d4T and ddI
(3).
Management of Occupational Exposure by Emergency Physicians
Although PHS guidelines for the management of occupational exposures to HIV were first published in 1985
(42), HCP often are not familiar with these guidelines. Focus groups conducted among emergency department (ED) physicians in
2002 indicated that of 71 participants, >95% had not read the 2001 guidelines before being invited to participate
(43). All physicians participating in these focus groups had managed occupational exposures to blood or body fluids. They cited
three challenges in exposure management most frequently: evaluation of an unknown source patient or a source patient who
refused testing, inexperience in managing occupational HIV exposures, and counseling of exposed workers in busy EDs.
Occupational HIV Exposure Management and PEP Use in U.S. Hospitals
Analysis of NaSH data for June 1995--December 2004 provides information regarding the management of
occupational exposure to HIV in a convenience sample of 95 U.S. hospitals. These data indicate improved adherence to
PHS recommendations concerning use of HIV PEP after occupational exposures. A total of 28,010 exposures to blood and
body fluids were reported by these hospitals (CDC, unpublished data, 2005). For all 25,510 exposures with known sources,
1,350 (5.3%) were to HIV-positive sources, 15,301 (60.0%) to HIV-negative sources, and 8,859 (34.7%) to sources of
unknown HIV status. Of 1,350 HCP exposed to a known HIV-positive source, 788 (58.4%) started PEP, and 317 (49%) of 647
for whom follow-up information was available took PEP for
>21 days. The overall median duration of HIV PEP after exposure
to an HIV-positive source was 27 days, increasing from 10 days in 1995 to 26.5 days in 2004; the overall median duration
of HIV PEP after exposure to an HIV-negative source was 2 days, decreasing from 7.5 days in 1995 to 1 day in 2004. The use
of rapid HIV tests for evaluation of source patients has increased; during 1995--1997, none of 25 NaSH facilities used
rapid HIV tests, whereas in 2004, a total of 21 (84% ) did (CDC, unpublished data, 2005). Rapid HIV tests could result
in decreased use of PEP and spare personnel both undue anxiety and adverse effects of antiretroviral PEP
(44--47). The annual median time to initiation of PEP was
consistent (2 hours). Of 1,350 HCP with exposures to HIV-positive sources,
909 (67.1%) had at least one follow-up serologic test recorded, but only 289 (31.8%) had tests recorded at 4--6 months
(CDC, unpublished data, 2005).
In 1996, of 24 HCP taking PEP after exposure to HIV-positive sources, 10 (42%) took a three-drug PEP regimen
compared with 30 (76.9%) of 39 in 2004 (CDC, unpublished data, 2005).
After 227 HIV exposures for which only a two-drug PEP regimen was recommended (i.e., the exposure was to mucous membranes or skin or was a superficial
percutaneous injury and the source person did not have end-stage AIDS or acute HIV illness), 104 (45.8%) HCP initiated a
three-drug HIV PEP regimen. The National Clinicians' Post-Exposure Prophylaxis Hotline
(PEPline)† reports similar findings.
PEPline staff recommended changing or discontinuing PEP regimens for 45 (38%) of 118 exposures involving source patients
with known viral load or CD4 cell count concerning which they were consulted during April 2002--March 2003
(48; R. Goldschmidt, PEPline, personal communication, 2004). For 14 (11.9%) HCP, the recommendation was to decrease
the number of drugs in the PEP regimens; for 22 (18.7%) HCP, the recommendation was to increase the number of drugs;
and for nine (7.6%), the recommendation was to change the PEP regimen, keeping the same number of drugs.
Recommendations for the Management of HCP Potentially Exposed to HIV
Exposure prevention remains the primary strategy for
reducing occupational bloodborne pathogen infections.
However, occupational exposures will continue to occur, and PEP will remain an important element of exposure management.
HIV PEP
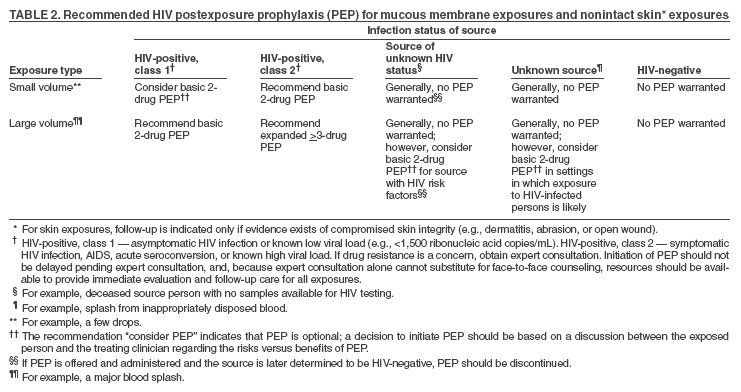
The recommendations provided in this report (Tables 1 and
2; Appendix) apply to situations in which HCP have
been exposed to a source person who either has or is considered likely to have HIV infection. These recommendations are based
on the risk for HIV infection after different types of exposure and on limited data regarding efficacy and toxicity of PEP. If PEP
is offered and taken and the source is later determined to be HIV-negative, PEP should be discontinued. Although
concerns have been expressed regarding HIV-negative sources being in the window period for seroconversion, no case of
transmission involving an exposure source during the window period has been reported in the United
States(39). Rapid HIV testing of source patients can facilitate making timely decisions regarding use of HIV PEP after occupational exposures to sources
of
unknown HIV status. Because the majority of occupational HIV exposures do not result in transmission of HIV,
potential toxicity must be considered when prescribing PEP. Because of the complexity of selecting HIV PEP regimens, when
possible, these recommendations should be implemented in consultation with persons having expertise in antiretroviral therapy
and HIV transmission. Reevaluation of exposed HCP should be strongly encouraged within
72 hours postexposure, especially as additional information about the exposure or source person becomes available.
Timing and Duration of PEP
PEP should be initiated as soon as possible, preferably within hours rather than days of exposure. If a question
exists concerning which antiretroviral drugs to use, or whether to use a basic or expanded regimen, the basic regimen should
be started immediately rather than delay PEP administration. The optimal duration of PEP is unknown. Because 4 weeks
of ZDV appeared protective in occupational and animal studies, PEP should be administered for 4 weeks, if tolerated
(49--52).
Recommendations for the Selection of Drugs for HIV PEP
The selection of a drug regimen for HIV PEP must balance the risk for infection against the potential toxicities of
the agent(s) used. Because PEP is potentially toxic, its use is not justified for exposures that pose a negligible risk for
transmission (Tables 1 and 2). The initial HIV PEP regimens recommended in these guidelines should be viewed as suggestions that can
be changed if additional information is obtained concerning
the source of the occupational exposure (e.g., possible
treatment history or antiretroviral drug resistance) or if expert consultation is provided. Given the complexity of choosing
and administering HIV PEP, whenever possible, consultation
with an infectious diseases consultant or another physician who
has experience with antiretroviral agents is recommended, but it should not delay timely initiation of PEP.
Consideration should be given to the comparative risk represented by the exposure and information regarding the
exposure source, including history of and response to antiretroviral therapy based on clinical response, CD4+ T-cell counts, viral
load measurements, and current disease stage. When the source person's virus is known or suspected to be resistant to one or
more of the drugs considered for the PEP regimen, the
selection of drugs to which the source person's virus is
unlikely to be resistant is recommended; expert consultation is advised. If this information is not immediately available, initiation of PEP, if
indicated, should not be delayed; changes in the regimen can be made after PEP has started, as appropriate. For HCP who initiate
PEP, re-evaluation of the exposed person should occur within 72 hours postexposure, especially if additional information about
the exposure or source person becomes available.
PHS continues to recommend stratification of HIV PEP regimens based on the severity of exposure and
other considerations (e.g., concern for antiretroviral drug resistance in the exposure source). The majority of HIV exposures
will warrant a two-drug regimen, using two NRTIs or one NRTI and one NtRTI (Tables 1 and
2; Appendix). Combinations
that can be considered for PEP include ZDV and 3TC or emtricitabine (FTC); d4T and 3TC or FTC; and tenofovir (TDF)
and 3TC or FTC. In the previous PHS guidelines, a combination of d4T and ddI was considered one of the first-choice
PEP regimens; however, this regimen is no longer recommended because of concerns about toxicity (especially neuropathy
and pancreatitis) and the availability of more tolerable
alternative regimens (3).
The addition of a third (or even a fourth) drug should be considered for exposures that pose an increased risk
for transmission or that involve a source in whom antiretroviral drug resistance is likely. The addition of a third drug for PEP
after a high-risk exposure is based on demonstrated effectiveness in reducing viral burden in HIV-infected persons. However,
no definitive data exist that demonstrate increased efficacy of three- compared with two-drug HIV PEP regimens.
Previously, IDV, nelfinavir (NFV), EFV, or abacavir (ABC) were recommended as first-choice agents for inclusion in an
expanded PEP regimen (3).
PHS now recommends that expanded PEP regimens be PI-based. The PI preferred for use in expanded PEP regimens
is lopinavir/ritonavir (LPV/RTV). Other PIs acceptable for use in expanded PEP regimens include atazanavir,
fosamprenavir, RTV-boosted IDV, RTV-boosted SQV, or NFV (Appendix). Although side effects are common with NNRTIs, EFV may
be considered for expanded PEP regimens, especially when resistance to PIs in the source person's virus is known or
suspected. Caution is advised when EFV is used in women of childbearing age because of the risk of
teratogenicity.
Drugs that may be considered as alternatives to the expanded regimens, with warnings about side effects and other
adverse events, are EFV or PIs as noted in the Appendix in combination with ddl and either 3TC or FTC. The fusion
inhibitor enfuvirtide (T20) has theoretic benefits for use in PEP
because its activity occurs before viral-host cell integration; however,
it
is not recommended for routine HIV PEP because of the mode of administration (subcutaneous injection twice
daily). Furthermore, use of T20 has the potential for production of anti-T20 antibodies that cross react with HIV gp41. This
could result in a false-positive, enzyme immunoassay (EIA) HIV antibody test among HIV-uninfected patients. A
confirmatory Western blot test would be expected to be negative in such cases. T20 should only be used with expert consultation.
Antiviral drugs not recommended for use as PEP, primarily because of the higher risk for potentially serious or
life-threatening adverse events, include ABC, delavirdine, ddC, and, as noted previously, the combination of ddI and d4T.
NVP should not be included in PEP regimens except with expert consultation because of serious reported side effects,
including hepatotoxicty (with one instance of fulminant liver failure requiring liver transplantation), rhabdomyolysis,
and hypersensitivity syndrome (53--55).
Because of the complexity of selection of HIV PEP regimens, consultation with persons having expertise in
antiretroviral therapy and HIV transmission is strongly recommended. Certain institutions have required consultation with a
hospital epidemiologist or infectious diseases consultant when HIV PEP use is under consideration. This can be especially important
in management of a pregnant or breastfeeding worker or a worker who has been exposed to a heavily
treatment-experienced source (Box 1).
Resources for consultation are available from the following sources:
HIV Antiretroviral Pregnancy Registry at
http://www.apregistry.com/index.htm; Address: Research Park, 1011 Ashes
Drive, Wilmington, NC 28405. Telephone: 800-258-4263; Fax: 800-800-1052; E-mail: registry@nc.crl.com;
FDA (for reporting unusual or severe toxicity to antiretroviral agents) at
http://www.fda.gov/medwatch; telephone:
800-332-1088; address: MedWatch, HF-2, Food and Drug Administration, 5600 Fishers Lane, Rockville, MD 20857;
CDC (for reporting HIV infections in HCP and failures of PEP) at telephone 800-893-0485; and
HCP with occupational exposure to HIV should receive follow-up counseling, postexposure testing, and medical
evaluation regardless of whether they receive PEP. HIV-antibody testing by enzyme immunoassay should be used to monitor HCP
for seroconversion for >6 months after occupational HIV exposure. After baseline testing at the time of exposure,
follow-up testing could be performed at 6 weeks, 12 weeks, and
6 months after exposure. Extended HIV follow-up (e.g., for 12
months) is recommended for HCP who become infected with HCV after exposure to a source coinfected with HIV and
HCV. Whether extended follow-up is indicated in other circumstances (e.g., exposure to a source co-infected with HIV and HCV
in the absence of HCV seroconversion or for exposed
persons with a medical history suggesting an impaired ability to mount
an antibody response to acute infection) is unclear. Although rare instances of delayed HIV
seroconversion have been reported (56,57), the infrequency of this occurrence does not warrant adding to exposed persons' anxiety by routinely extending
the duration of postexposure follow-up. However, this should not preclude a decision to extend
follow-up in a particular situation based on the clinical judgment of the exposed person's health-care provider. The routine use of direct virus assays (e.g.,
HIV p24 antigen EIA or tests for HIV ribonucleic acid) to detect infection among exposed HCP usually is not recommended
(58). Despite the ability of direct virus assays to detect HIV infection a few days earlier than EIA, the infrequency of
occupational seroconversion and increased costs of these tests do not warrant their routine use in this setting. In addition, the relatively
high rate of false-positive results of these tests in this setting could lead to unnecessary anxiety or treatment
(59,60). Nevertheless, HIV testing should be performed on any
exposed person who has an illness compatible with an acute retroviral
syndrome, regardless of the interval since exposure. A person in whom HIV infection is identified should be
referred for medical management to a specialist with expertise in HIV treatment and counseling.
Health-care providers caring for persons with occupationally acquired HIV infection can report these cases to CDC at telephone 800-893-0485 or to their state
health departments.
Monitoring and Management of PEP Toxicity
If PEP is used, HCP should be monitored for drug toxicity by testing at baseline and again 2 weeks after starting PEP.
The scope of testing should be based on medical conditions in the exposed person and the toxicity of drugs included in the
PEP regimen. Minimally, laboratory monitoring for toxicity should include a complete blood count and renal and hepatic
function tests. Monitoring for evidence of hyperglycemia should be included for HCP whose regimens include any PI; if the
exposed person is receiving IDV, monitoring for crystalluria, hematuria, hemolytic anemia, and hepatitis also should be included.
If toxicity is noted, modification of the regimen should be considered after expert consultation;
further diagnostic studies might be indicated.
Exposed HCP who choose to take PEP should be advised of the importance of completing the prescribed
regimen. Information should be provided about potential drug
interactions and drugs that should not be taken with PEP, side effects
of prescribed drugs, measures to minimize side effects, and methods of clinical monitoring for toxicity
during the follow-up period. HCP should be advised that evaluation of certain symptoms (e.g., rash, fever, back or abdominal pain, pain
on urination or blood in the urine, or symptoms of hyperglycemia (e.g., increased thirst or frequent urination) should not
be delayed.
HCP often fail to complete the recommended regimen
often because they experience side effects (e.g., nausea or
diarrhea). These symptoms often can be managed with antimotility and antiemetic agents or other medications that target
specific symptoms without changing the regimen. In other situations, modifying the dose interval (i.e., administering a lower dose
of drug more frequently throughout the day, as recommended by the manufacturer) might facilitate
adherence to the regimen. Serious adverse
events§ should be reported to FDA's MedWatch program.
Although recommendations for follow-up testing, monitoring, and counseling of exposed HCP are unchanged from
those published previously (3), greater emphasis is needed on improving follow-up care provided to exposed HCP (Box 2).
This might result in increased adherence to HIV PEP regimens, better management of associated symptoms with
ancillary medications or regimen changes, improved detection of serious adverse effects, and serologic testing among a larger
proportion of exposed personnel to determine if infection is transmitted after occupational exposures. Closer follow-up should in
turn reassure HCP who become anxious after these events
(61,62). The psychologic impact on HCP of needlesticks or exposure
to blood or body fluid should not be underestimated. Providing HCP with psychologic counseling should be an
essential component of the management and care of exposed HCP.
Reevaluation and Updating of HIV PEP Guidelines
As new antiretroviral agents for treatment of HIV infection and additional information concerning early HIV infection
and prevention of HIV transmission become available, the PHS Interagency Working Group will assess the need to
update these guidelines. Updates will be published periodically as appropriate.
Acknowledgments
David K. Henderson, MD, National Institutes of Health, Bethesda, Maryland; Kimberly A. Struble, PharmD, Food and
Drug Administration, Rockville, Maryland; and Abe Macher, MD, Health Resources and Services Administration, Rockville, Maryland,
assisted in the preparation of this report.
US Department of Health and Human Services Public Health Service Task Force. Recommendations for use of antiretroviral drugs in
pregnant HIV-1 infected women for maternal health and Interventions to reduce perinatal HIV-1 transmission in the United States. Available at
http://www.aidsinfo.nih.gov/guidelines/default_db2.asp?id=66.
Havens PL; Committee on Pediatric AIDS. Postexposure prophylaxis in children and adolescents for nonoccupational exposure to
human immunodeficiency virus. Pediatrics 2003;111:1475--89.
Bell DM. Occupational risk of human immunodeficiency virus
infection in health-care workers: an overview. Am J Med 1997;102(5B):9--15.
Wahn V, Kramer HH, Voit T, Bruster HT, Scrampical B, Scheid A. Horizontal transmission of HIV infection between two
siblings. Lancet 1986;ii:694.
Anonymous. Transmission of HIV by human bite. Lancet 1987;ii:522.
Richman KM, Rickman LS. The potential for transmission of human immunodeficiency virus through human bites. J Acquir Immune Defic
Syndr 1993;6:402--6.
Vidmar L, Poljak M, Tomazic J, Seme K, Klavs I. Transmission of HIV-1 by human bite. Lancet 1996;347:1762.
Pretty IA, Anderson GS, Sweet DJ. Human bites and the risk of
human immunodeficiency virus transmission. Am J Forensic Med Pathol 1999;20:232--9.
Panel on Clinical Practices for Treatment of HIV Infection. Guidelines for the use of antiretroviral agents in HIV-infected adults and
adolescents---April 7, 2005. Bethesda, MD: National Institutes of Health; 2005. Available at
http://aidsinfo.nih.gov/guidelines/default_db2.asp?id=50.
Yeni PG, Hammer SM, Hirsch MS, et al. Treatment for adult HIV infection: 2004 recommendations of the International AIDS Society-USA
Panel. JAMA 2004;292:251--65.
Wang SA, Panlilio AL, Doi PA, et al. Experience of health-care workers taking postexposure prophylaxis after occupational
human immunodeficiency virus exposures: findings of the HIV Postexposure Prophylaxis Registry. Infect Control Hosp Epidemiol 2000;21:780--5.
Swotinsky RB, Steger KA, Sulis C, Snyder S, Craven DE. Occupational exposure to HIV: experience at a tertiary care center. J Occup Environ
Med 1998;40:1102--9.
Parkin JM, Murphy M, Anderson J, El-Gadi S, Forster G, Pinching AJ. Tolerability and side-effects of post-exposure prophylaxis for HIV
infection. Lancet 2000;355:722--3.
Puro V. Post-exposure prophylaxis for HIV infection [Letter]. Lancet 2000;355:1556--7.
Lee LM, Henderson DK. Tolerability of postexposure antiretroviral
prophylaxis for occupational exposures to HIV. Drug Saf 2001;24:587--97.
Russi M, Buitrago M, Goulet J, et al. Antiretroviral prophylaxis of health care workers at two urban medical centers. J Occup Environ
Med 2000;42:1092--100.
Garb JR. One-year study of occupational human immunodeficiency
virus postexposure prophylaxis. J Occup Environ Med 2002;44:265--70.
Grime PR, Risi L, Binns C, Carruthers JR, Williams S. Pan-Thames survey of occupational exposure to HIV and the use of
post-exposure prophylaxis in 71 NHS trusts. J Infect 2001;42:27--32.
Puro V, DeCarli G, Soldani F, et al. Adverse drug reactions associated with PEP [Poster]. In: Program and Abstracts of the 10th Conference
on Retroviruses and Opportunistic Infections, Boston, Massachusetts, February 2003. Poster no. 711.
Moyle G, Boffito M. Unexpected drug interactions and adverse events with antiretroviral drugs. Lancet 2004;364:8--10.
Andrade A, Flexner C. Progress in pharmacology and drug interactions from the 10th CROI. Hopkins HIV Rep 2003;15:7,11.
Andrade A, Flexner C. Genes, ethnicity, and efavirenz response: clinical pharmacology update from the 11th CROI. Hopkins HIV Rep
2004;16:1--7.
de Maat MM, Ekhart GC, Huitema AD, Koks CH, Mulder JW, Beijnen JH. Drug interactions between antiretroviral drugs and
comedicated agents. Clin Pharmacokinet 2003;42:223--82.
Fichtenbaum CJ, Gerber JG. Interactions between antiretroviral drugs and drugs used for the therapy of the metabolic
complications encountered during HIV infection. Clin Pharmacokinet 2002;41:1195--211.
Edmunds-Obguokiri T. Understanding drug-drug interactions in the management of HIV disease. HIV Clin 2002;14:1--4.
Rainey PM. HIV drug interactions: the good, the bad, and the other. Ther Drug Monit 2002;24:26--31.
Dasgupta A, Okhuysen PC. Pharmacokinetic and other drug interactions in patients with AIDS. Ther Drug Monit 2001;23:591--605.
Piscitelli SC, Gallicano KD. Interactions among drugs for HIV and opportunistic infections. N Engl J Med 2001;334:984--96.
Gerberding JL. Occupational exposure to HIV in health care settings. N Engl J Med 2003;348:826--33.
Bassett IV, Freedberg KA,Walensky RP. Two drugs or three? Balancing efficacy, toxicity, and resistance in postexposure prophylaxis for
occupational exposure to HIV. Clin Infect Dis 2004;39:395--401.
Beltrami EM, Cheingsong R, Heneine WM, et al. Antiretroviral drug resistance in human immunodeficiency virus--infected source patients
for occupational exposures to healthcare workers. Infect Control Hosp Epidemiol 2003;24:724--30.
Hirsch MS, Brun-Vezinet F, Clotet B, et al. Antiretroviral drug resistance testing in adults infected with human immunodeficiency virus type
1: 2003 recommendations of an International AIDS Society-USA Panel. Clin Infect Dis 2003;37:113--28.
Hawkins DA, Asboe D, Barlow K, Evans B. Seroconversion to HIV-1 following a needlestick injury despite combination post-exposure
prophylaxis. J Infect 2001;43:12--8.
Do AN, Ciesielski CA, Metler RP, Hammett TA, Li J, Fleming PL. Occupationally acquired human immunodeficiency virus (HIV)
infection: national case surveillance data during 20 years of the HIV epidemic in the United States. Infect Control Hosp Epidemiol 2003;24:86--96.
Health Protection Agency Centre for Infections and Collaborators. Occupational transmission of HIV: summary of published reports. March
2005 edition. Data to the end of December 2002. London, UK: Health Protection Agency Centre for Infections and Collaborators. Available at
http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/occupational.htm.
Puro V. Genotypic resistance tests for the management of postexposure prophylaxis. Scand J Infect Dis Suppl 2003;(35 Suppl):106:93--8.
Panlilio AL, Sinkowitz-Cochran R, Grady MA, Cardo DM. Barriers to and facilitators of implementing U.S. Public Health Service (PHS)
guidelines on occupational exposure management by emergency physicians [Abstract]. In: Program and Abstracts of the 13th annual meeting of the Society
for Health-care Epidemiology of America, Arlington, Virginia, April 5--8, 2003. Abstract no. 240.
Kallenborn JC, Price TG, Carrico R, Davidson AB. Emergency
department management of occupational exposures: cost analysis of rapid HIV
test. Infect Control Hosp Epidemiol 2001;22:289--93.
King AM, Osterwalder JJ, Vernazza PL. A randomised prospective study to evaluate a rapid HIV-antibody assay in the management of cases
of percutaneous exposure amongst health care workers. Swiss Med Wkly 2001;131:10--3.
Salgado CD, Flanagan HL, Haverstick DM, Farr BM. Low rate of false-positive results with use of a rapid HIV test. Infect Control Hosp
Epidemiol 2002;23:335--7.
Puro V, Francisci D, Sighinolfi L, et al. Benefits of a rapid HIV test for evaluation of the source patient after occupational exposure of
health-care workers. J Hosp Infect 2004;57:179--82.
Dong BJ, Harvey A, Aranow RA, et al. Post-exposure prophylaxis (PEP) in health care workers (HCWs) after exposure to an HIV-infected
source patient (SP) [Poster]. In: Program and Abstract of the 11th Conference on Retroviruses and Opportunistic Infections, San Francisco,
California, February 8--11, 2004. Poster no. 887.
Shih C-C, Kaneshima H, Rabin L, et al. Postexposure prophylaxis with zidovudine suppresses human immunodeficiency virus type 1 infection
in SCID-hu mice in a time-dependent manner. J Infect Dis 1991;163:625--7.
Tsai C-C, Follis KE, Sabo A, et al. Prevention of SIV infection in macaques by (R)-9-(2-phosphonylmethoxypropyl) adenine.
Science 1995;270:1197--9.
Tsai C-C, Emau P, Follis KE, et al. Effectiveness of postinoculation (R)-9-(2-phosphonylmethoxypropyl) adenine treatment for prevention
of persistent simian immunodeficiency virus
SIVmne infection depends critically on timing of initiation and duration of treatment. J
Virol 1998;72:4265--73.
Otten RA, Smith DK, Adams DR, et al. Efficacy of postexposure
prophylaxis after intravaginal exposure of pig-tailed macaques to a
human-derived retrovirus (human immunodeficiency virus type 2).
J Virol 2000;74:9771--5.
Cattelan AM, Erne E, Slatino A, et al. Severe hepatic failure related to nevirapine treatment. Clin Infect Dis 1999;29:455--6.
Johnson S, Baraboutis JG, Sha BE, Proia LA, Kessler HA. Adverse effects associated with use of nevirapine in HIV postexposure for
2 health care workers [Letter]. JAMA 2000;284:2722--3.
Ridzon R, Gallagher K, Ciesielski C, et al. Simultaneous transmission of human immunodeficiency virus and hepatitis C virus from a
needle-stick injury. N Engl J Med 1997;336:919--22.
Ciesielski CA, Metler RP. Duration of time between exposure and seroconversion in healthcare workers with occupationally acquired
infection with human immunodeficiency virus. Am J Med 1997;102(Suppl 5B):115--6.
Busch MP, Satten GA. Time course of viremia and antibody seroconversion following human immunodeficiency virus exposure. Am J
Med 1997;102(Suppl 5B):117--24.
Rich JD, Merriman NA, Mylonakis E, et al. Misdiagnosis of HIV
infection by HIV-1 plasma viral load testing: a case series. Ann Intern
Med 1999;130:37--9.
Roland ME, Elbeik TA, Kahn JO, et al. HIV RNA testing in the context of nonoccupational postexposure prophylaxis. J Infect Dis
2004;190:598--604.
Armstrong K, Gorden R, Santorella G. Occupational exposure of health carMorbidity
and Mortality Weekly Report (MMWR)e workers (HCWs) to human immunodeficiency virus (HIV):
stress reactions and counseling interventions. Social Work in Health Care 1995;21:61--80.
Meienberg F, Bucher HC, Sponagel L, Zinkernagel C, Gyr N, Battegay M. Anxiety in health care workers after exposure to potentially
HIV-contaminated blood or body fluids. Swiss Med Wkly 2002;132:321--4.
Food and Drug Administration. 21CFR314.80. Postmarketing reporting of adverse drug experiences. Code of Federal Regulations 2005;5:114--7.
* This interagency working group included representatives from CDC, FDA, the Health Resources and Services Administration, and the National Institutes
of Health. Information included in these recommendations might not represent FDA approval or approved labeling for the particular product or indications
in question. Specifically, the terms "safe" and "effective" might not be synonymous with the FDA-defined legal standard for product approval.
† Administered by staff members from the University of California at San Francisco and San Francisco General Hospital; supported by the Health Resources
and Services Administration Ryan White CARE Act and AIDS Education and Training Centers, and by CDC.
§ Defined by FDA as follows: "Any adverse drug experience occurring at any dose that results in any of the following outcomes: death, a life-threatening
adverse drug experience, inpatient hospitalization or prolongation of existing hospitalization, a persistent or significant disability/incapacity, or a congenital
anomaly/birth defect. Important medical events that may not result in death, be life-threatening, or require hospitalization may be considered a serious adverse
drug experience when, based upon appropriate medical judgment, they may jeopardize the patient or subject and may require medical or surgical intervention
to prevent one of the outcomes listed in this definition"
(63).
Basic and Expanded HIV Postexposure Prophylaxis Regimens
BASIC REGIMEN
Zidovudine (Retrovir™; ZDV; AZT) + lamivudine
(Epivir®; 3TC); available as Combivir™
<>
Preferred dosing
--- ZDV: 300 mg twice daily or 200 mg three times daily, with food; total: 600 mg daily
--- 3TC: 300 mg once daily or 150 mg twice daily
--- Combivir: one tablet twice daily
--- ZDV associated with decreased risk for HIV
transmission --- ZDV used more often than other drugs for PEP for health-care personnel (HCP)
--- Serious toxicity rare when used for PEP
--- Side effects predictable and manageable with antimotility and antiemetic agents
--- Can be used by pregnant HCP --- Can be given as a single tablet (COMBIVIR™) twice daily
Disadvantages
--- Side effects (especially nausea and fatigue) common and might result in low adherence
--- Source-patient virus resistance to this regimen
possible
--- Potential for delayed toxicity (oncogenic/teratogenic) unknown
--- ZDV: 300 mg twice daily or 200 mg three times daily, with food; total:
600 mg/day, in 2--3 divided doses
--- FTC: 200 mg (one capsule) once daily
Dosage forms
--- ZDV: see above
--- FTC: 200 mg capsule
FTC general comments
--- Nucleoside analogue; same structure as 3TC, except fluoride residue at position 5 on pyrimidine ring
--- Same resistance and safety profile as 3TC
--- No apparent advantage over 3TC; tolerability and virologic response rates appear better than regimens containing
ddI + d4T
Advantages
--- ZDV: see above.
--- FTC
o Convenient (once daily)
o Well tolerated
o Long intracellular half-life (~40 hours)
Disadvantages
--- ZDV: see above.
--- FTC
o Rash perhaps more frequent than with 3TC
o No long-term experience with this drug
o Cross resistance to 3TC
o Hyperpigimentation among non-Caucasians with long-term use: 3%
--- TDF: 300 mg once daily
--- 3TC: 300 mg once daily or 150 mg twice daily
Dosage forms
--- TDF: 300 mg tablet
--- 3TC: see above
Advantages
--- 3TC: see above
--- TDF
o Convenient dosing (single pill once daily)
o Resistance profile activity against certain
thymidine analogue mutations
o Well tolerated
Disadvantages
--- TDF
o Same class warnings as nucleoside reverse
transcriptase inhibitors (NRTIs)
o Drug interactions
o Increased TDF concentrations among persons
taking atazanavir and lopinavir/ritonavir; need to monitor
patients for TDF-associated toxicities
--- Preferred dosage of atazanavir if used with TDF: 300 mg + ritonavir 100 mg once daily + TDF 300 mg once daily
Tenofovir DF
(Viread®; TDF) + emtricitabine
(Emtriva™; FTC); available as
Truvada™
Preferred dosing
--- TDF: 300 mg once daily
--- FTC: 200 mg once daily
--- As Truvada™: one tablet daily
Dosage forms
--- TDF: 300 mg tablet
--- FTC: see FTC
--- Truvada™ (TDF 300 mg plus FTC 200 mg)
Advantages
--- FTC: see above
--- TDF
o Convenient dosing (single pill once daily)
o Resistance profile activity against certain
thymidine analogue mutations
o Well tolerated
Disadvantages
--- TDF
o Same class warnings as NRTIs
o Drug interactions
o Increased TDF concentrations among persons taking atazanavir and lopinavir/ritonavir; need to monitor
patients for TDF-associated toxicities
o Preferred dosing of atazanavir if used with TDF: 300 mg + ritonavir 100 mg once daily + TDF 300 mg once daily
--- 3TC: 300 mg once daily or 150 mg twice daily
--- d4T: 40 mg twice daily (can use lower doses of 20--30 mg twice daily if toxicity occurs; equally
effective but less toxic among HIV-infected patients with peripheral neuropathy); 30 mg twice daily if body weight is <60 kg
Dosage forms
--- 3TC: see above
--- d4T: 15, 20, 30, and 40 mg tablet
Advantages
--- 3TC: see above
--- d4T: gastrointestinal (GI) side effects rare
Disadvantages
--- Possibility that source-patient virus is resistant to this regimen
--- Potential for delayed toxicity (oncogenic/teratogenic) unknown
--- FTC: 200 mg daily
--- d4T: 40 mg twice daily (can use lower doses of
20--30 mg twice daily if toxicity occurs; equally effective but less
toxic among HIV-infected patients who developed peripheral neuropathy); if body weight is
<60 kg, 30 mg twice daily
Dosage forms
--- FTC: see above
--- d4T: see above
Advantages
--- 3TC and FTC: see above; d4T's GI side effects rare
Disadvantages
--- Potential that source-patient virus is resistant to this regimen
--- Unknown potential for delayed toxicity (oncogenic/teratogenic) unknown
--- 3TC: 300 mg once daily or 150 mg twice daily
--- ddI: Videx® chewable/dispersible buffered tablets can be administered on an empty stomach as either 200 mg
twice daily or 400 mg once daily. Patients must take at least two of the appropriate strength tablets at each dose to
provide adequate buffering and prevent gastric acid degradation of ddI. Because of the need for adequate buffering, the
200-mg strength tablet should be used only as a component of a once-daily regimen. The dose is either 200 mg twice
daily or 400 mg once daily for patients weighing >60 kg and 125 mg twice daily or 250 mg once daily for
patients weighing >60 kg.
Dosage forms
--- 3TC: 150 or 300 mg tablets
--- ddI: 25, 50, 100, 150, or 200 mg buffered white tablets
Advantages
--- ddI: once daily dosing option
--- 3TC: see above
Disadvantages
--- Tolerability: diarrhea more common with buffered preparation than with enteric-coated preparation
--- Associated with toxicity: peripheral neuropathy, pancreatitis, and lactic acidosis
--- Must be taken on empty stomach except with TDF
--- Drug interactions
--- 3TC: see above
--- Tolerability: diarrhea more common with buffered than with enteric-coated preparation
--- Associated with toxicity: peripheral neuropathy,
pancreatitis, and lactic acidosis
--- Must be taken on empty stomach except with TDF
--- Drug interactions
--- FTC: see above
--- Potent HIV protease inhibitor
--- Generally well-tolerated
Disadvantages
--- Potential for serious or life-threatening drug interactions (see
Table 4)
--- Might accelerate clearance of certain drugs, including oral contraceptives (requiring alternative or
additional contraceptive measures for women taking these drugs)
--- Can cause severe hyperlipidemia, especially hypertriglyceridemia
--- GI (e.g., diarrhea) events common
--- ATV: 400 mg once daily, unless used in combination with TDF, in which case ATV should be boosted with
RTV, preferred dosing of ATV 300 mg + RTV: 100 mg once daily
--- Potent HIV protease inhibitor
--- Convenient dosing -- once daily
--- Generally well tolerated
Disadvantages
--- Hyperbilirubinemia and jaundice common
--- Potential for serious or life-threatening drug interactions (see
Table 4)
--- Avoid coadministration with proton pump inhibitors
--- Separate antacids and buffered medications by 2 hours and H2-receptor antagonists by 12 hours to avoid
decreasing ATV levels
--- Caution should be used with ATV and products known to induce PR prolongation (e.g., diltiazem)
--- Tolerability: GI side effects common
--- Multiple drug interactions. Oral contraceptives
decrease fosamprenavir concentrations
--- Incidence of rash in healthy volunteers, especially when used with low doses of ritonavir. Differentiating between
early drug-associated rash and acute seroconversion can be difficult and cause extraordinary concern for the exposed person
--- Potential for serious or life-threatening drug interactions (see
Table 4)
--- Serious toxicity (e.g., nephrolithiasis) possible;
consumption of 8 glasses of fluid/day required
--- Hyperbilirubinemia common; must avoid this drug during late pregnancy
--- Requires acid for absorption and cannot be taken
simultaneously with ddI, chewable/dispersible buffered
tablet formulation (doses must be separated by >1 hour)
--- Does not require phosphorylation before activation and might be active earlier than other antiretroviral agents
(a theoretic advantage of no demonstrated clinical benefit)
--- Once daily dosing
Disadvantages
--- Drug associated with rash (early onset) that can be severe and might rarely progress to Stevens-Johnson syndrome
--- Differentiating between early drug-associated rash and acute seroconversion can be difficult and
cause extraordinary concern for the exposed person
--- Central nervous system side effects (e.g., dizziness, somnolence, insomnia, or abnormal dreaming) common;
severe psychiatric symptoms possible (dosing before bedtime might minimize these side effects)
--- Teratogen; should not be used during pregnancy
--- Potential for serious or life-threatening drug interactions (see
Table 5)
ANTIRETROVIRAL AGENTS GENERALLY NOT RECOMMENDED
FOR USE AS PEP
Nevirapine
(Viramune®; NVP)
Disadvantages
--- Associated with severe hepatotoxicity (including at least one case of liver failure requiring liver transplantation in
an exposed person taking PEP)
--- Associated with rash (early onset) that can be severe and progress to Stevens-Johnson syndrome
--- Differentiating between early drug-associated rash and acute seroconversion can be difficult and
cause extraordinary concern for the exposed person
--- Drug interactions: can lower effectiveness of certain antiretroviral agents and other commonly used
medicines
Delavirdine
(Rescriptor®; DLV)
Disadvantages
--- Drug associated with rash (early onset) that can be severe and progress to Stevens-Johnson syndrome
--- Multiple drug interactions
Abacavir (Ziagen®; ABC)
Disadvantages
--- Severe hypersensitivity reactions can occur, usually within the first 6 weeks
--- Differentiating between early drug-associated rash/hypersensitivity and acute seroconversion can be
difficult
Zalcitabine (Hivid®; ddC)
Disadvantages
--- Three times a day dosing
--- Tolerability
--- Weakest antiretroviral agent
ANTIRETROVIRAL AGENT FOR USE AS PEP ONLY WITH EXPERT CONSULTATION
--- T20: Single-dose vial, reconstituted to 90 mg/ml
Advantages
--- New class
--- Unique viral target; to block cell entry
--- Prevalence of resistance low
Disadvantages
--- Twice-daily injection
--- Safety profile: local injection site reactions
--- Never studied among antiretroviral-naïve or HIV-negative patients
--- False-positive EIA HIV antibody tests might result from formation of anti-T20 antibodies that cross-react with
anti-gp41 antibodies
PHS Working Group on Occupational Postexposure
Prophylaxis: Adelisa L Panlilio, Denise M. Cardo, Division of Healthcare Quality
Promotion, National Center for Infectious Diseases, CDC; Lisa A. Grohskopf; Walid Heneine, Division of HIV/AIDS Prevention, National Center for HIV,
STD, and TB Prevention, CDC; Clara Sue Ross, Ahmed Gomaa; Division of Surveillance and Hazard Evaluations, and Field Studies, National Institute
for Occupational Safety and Health, CDC; Kimberly A. Struble, Center for Drug Evaluation and Research, FDA; Abe Macher, HIV/AIDS Bureau,
HRSA; David K Henderson, Clinical Center, National Institutes of Health.
External Consultants: Henry M. Blumberg, Grady Memorial Hospital; Betty Dong, National Clinicians' Postexposure Prophylaxis Hotline
(PEPline); Ron Goldschmidt, University of California, San Francisco; Michael Saag, University of Alabama, Birmingham; Michael Tapper, Lenox Hill Hospital.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.