Timothy H. Holtz, M.D., M.P.H.1,2 S. Patrick Kachur, M.D., M.P.H.2 John R. MacArthur, M.D., M.P.H.1,2
Jacquelin M. Roberts, M.S.2 Ann M. Barber2 Richard W. Steketee, M.D., M.P.H.2 Monica E. Parise M.D.2
1Epidemic Intelligence Service, Epidemiology Program Office
2Division of Parasitic Diseases, National Center for Infectious Diseases
Abstract
Problem/Condition: Human malaria is caused by one or more of four species
of intraerythrocytic protozoa of the genus
Plasmodium (i.e., P. falciparum, P.
vivax, P. ovale, or P. malariae). The protozoa are transmitted by the bite of an
infective female Anopheles species mosquito. The majority of malaria infections in
the United States occur among persons who have traveled to areas with
endemic transmission. Cases occasionally occur that are acquired through exposure
to infected blood products, by congenital transmission, or by local
mosquitoborne transmission. Malaria surveillance is conducted to identify episodes of
local transmission and to guide prevention recommendations for travelers.
Reporting Period: Cases with an onset of symptoms during 1998.
Description of System: Malaria cases confirmed by blood smear are reported
to local and state health departments by healthcare providers and laboratory
staff members. Case investigations are conducted by local and state health
departments, and reports are sent to CDC through the National Malaria Surveillance
System (NMSS). This report uses NMSS data.
Results: CDC received reports of 1,227 cases of malaria with onsets of symptoms
in 1998, among persons in the United States and its territories. This number
represents a decrease of 20.5% from the 1,544 cases reported during 1997.
P. falciparum, P. vivax, P.
malariae, and P. ovale were identified in 42.8%, 37.8%, 3.5%, and 2.1%
of cases, respectively. More than one species was present in seven patients (0.6%
of total). The infecting species was not determined in 162 (13.2%) cases.
Compared with reported cases in 1997, reported malaria cases acquired in
Africa increased by 1.3% (n = 706); those acquired in Asia decreased by 52.1% (n =
239); and those acquired in the Americas decreased by 6.5% (n = 229). Of 636
U.S. civilians who acquired malaria abroad, 126 (19.8%) reportedly had followed
a chemoprophylactic drug regimen recommended by CDC for the area to which
they had traveled.
Five persons became infected in the United States. One case was
congenitally acquired; one was acquired by blood transfusion; and three were isolated cases
that could not be epidemiologically linked to another case. Four deaths were
attributed to malaria.
Interpretation: The 20.5% decrease in malaria cases during 1998 compared
with 1997 resulted primarily from decreases in P.
vivax cases acquired in Asia among non-U.S. civilians. This decrease could have resulted from local changes in
disease
transmission, decreased immigration from the region, decreased travel to
the region, incomplete reporting from state and local health departments, or
increased use of effective antimalarial chemoprophylaxis. In a majority of reported cases,
U.S. civilians who acquired infection abroad had not taken an
appropriate chemoprophylaxis regimen for the country where they acquired malaria.
Public Health Actions Taken: Additional information was obtained from state
and local health departments and clinics concerning the four fatal cases and the
five infections acquired in the United States. Persons traveling to a malarious
area should take a recommended chemoprophylaxis regimen and use
personal protection measures to prevent mosquito bites. Any person who has been to
a malarious area and subsequently develops fever or influenza-like symptoms
should seek medical care immediately; the investigation should include a blood smear
for malaria. Malaria infections can be fatal if not diagnosed and treated
promptly. Current recommendations concerning prevention and treatment of malaria can
be obtained from CDC.
INTRODUCTION
Human malaria is caused by infection with one or more of four species
of Plasmodium parasites (i.e., P.
falciparum, P. vivax, P. ovale, and
P. malariae). The infection is transmitted by the bite of an infective female
Anopheles species mosquito. Malaria remains a global problem, with an estimated 300--500
million cases occurring annually. A total of 41% of the world's population lives in
areas where malaria is transmitted regularly (e.g., parts of Africa, Asia, the Middle
East, Central and South America, Hispaniola, and Oceania), and approximately
1.5--2.7 million persons die of malaria each year
(1).
Malaria was also endemic throughout a majority of the continental United
States during the 1900s. Approximately 600,000 cases occurred in 1914
(2). During the late 1940s, a combination of improved socioeconomic conditions, water
management, vector-control efforts, and case management was successful in interrupting
malaria transmission in the United States. Subsequently, malaria case surveillance has
been maintained to detect locally acquired cases that could indicate the reintroduction
of transmission, and to monitor patterns in antimalarial drug resistance that
guide prevention recommendations for U.S. travelers.
The majority of malaria cases diagnosed in the United States are imported
from regions of the world where malaria transmission is known to occur. However,
each year congenital infections and infections resulting from exposure to blood or
blood products are reported in the United States. Cases also are reported that might
have been acquired through local mosquitoborne transmission
(3,4).
State and local health departments and CDC investigate all malaria cases acquired
in the United States, and CDC analyzes all imported cases to detect trends
in acquisition. This information is used to guide malaria prevention
recommendations for travelers abroad. For example, an increase in
P. falciparum malaria among U.S. travelers to Africa, an area with increasing chloroquine resistance, prompted CDC
to change the recommended chemoprophylaxis for Africa in 1990
(5).
The signs and symptoms of malaria are variable, but a majority of patients
have fever. Other common symptoms include headache, back pain, chills,
increased sweating, myalgia, nausea, vomiting, diarrhea, and cough. Malaria should
be considered when any of these symptoms occurs in a person who has traveled to
an
area endemic for malaria transmission. Malaria also should be considered in
the differential diagnosis for persons with fever of unknown origin, regardless of
their travel history. Untreated P.
falciparum infection can rapidly progress to coma,
renal failure, pulmonary edema, and death. Asymptomatic parasitemia can occur
among persons who have been long-term residents of malarious areas. This
report summarizes malaria cases reported to CDC that had onsets of symptoms
during 1998.
METHODS
Sources of Data
Data regarding malaria cases are reported to the National Malaria
Surveillance System (NMSS) and the National Notifiable Diseases Surveillance System
(NNDSS) (6). Although both systems rely on passive reporting, reported case numbers
might differ because of differences in data collection and transmission. A
substantial difference in the data collected in these two systems is that NMSS receives
more detailed clinical and epidemiologic data regarding each case (e.g.,
information concerning the area in which the infected person traveled). Cases of
blood-smear--confirmed malaria are identified by healthcare providers and laboratories.
Each slide-confirmed case is reported to local and state health departments and to CDC
on a uniform case report form that contains clinical, laboratory, and
epidemiologic information. CDC staff members review all report forms at the time of receipt
and request additional information if necessary (e.g., when no recent travel to
a malarious country is reported). Reports of other cases are telephoned directly to
CDC by health-care providers, usually when assistance with diagnosis or treatment
is requested. All cases acquired in the United States are investigated, including
all induced and congenital cases and possible introduced or cryptic cases.
Information derived from uniform case report forms is entered into a database and
analyzed annually.
Definitions
The following definitions are used in this report:
Laboratory criteria for
diagnosis: Demonstration of malaria parasites
on blood films.
Confirmed
case: Symptomatic or asymptomatic infection that occurs in
the United States in a person who has microscopically confirmed malaria
parasitemia, regardless of whether the person had previous attacks of malaria while in
other countries. A subsequent attack of malaria occurring in a person is counted as
an additional case if the demonstrated
Plasmodium species differ from the
initially identified species. A subsequent attack of malaria occurring in a person while in
the United States could indicate a relapsing infection or treatment failure,
possibly resulting from drug resistance, if the demonstrated
Plasmodium species is the same species identified previously, and is not counted as an additional case.
This report also uses terminology derived from World Health
Organization recommendations (7). Definitions of these terms are included for reference.
Autochthonous malaria:
Indigenous. Mosquitoborne transmission of malaria in an area
where malaria occurs regularly.
Introduced. Mosquitoborne transmission of malaria from an imported
case in an area where malaria does not occur regularly.
Imported
malaria: Malaria acquired outside a specific area. In this
report, imported cases are those acquired outside the United States and its
territories (including Puerto Rico, Guam, and the U.S. Virgin Islands).
Induced malaria: Malaria acquired through hematogenous means (e.g.,
blood transfusion or use of shared syringes).
Relapsing
malaria: Renewed manifestations (i.e., clinical symptoms
and parasitemia) from a previous malaria infection reoccurring at a longer interval
than is typical of the infection.
Cryptic malaria: An isolated malaria case that cannot be
linked epidemiologically to secondary cases.
Microscopic Diagnosis of Malaria
Early diagnosis of malaria requires that physicians consider malaria for every
patient who has fever; evaluation of such a patient should include a comprehensive
travel history. If malaria is suspected, a Giemsa-stained smear of the patient's
peripheral blood should be examined for parasites. Thick and thin blood smears must
be prepared properly because the accuracy of diagnosis depends on the quality of
the blood smear and the experience of the laboratory personnel *(Appendix
A).
RESULTS
General Surveillance
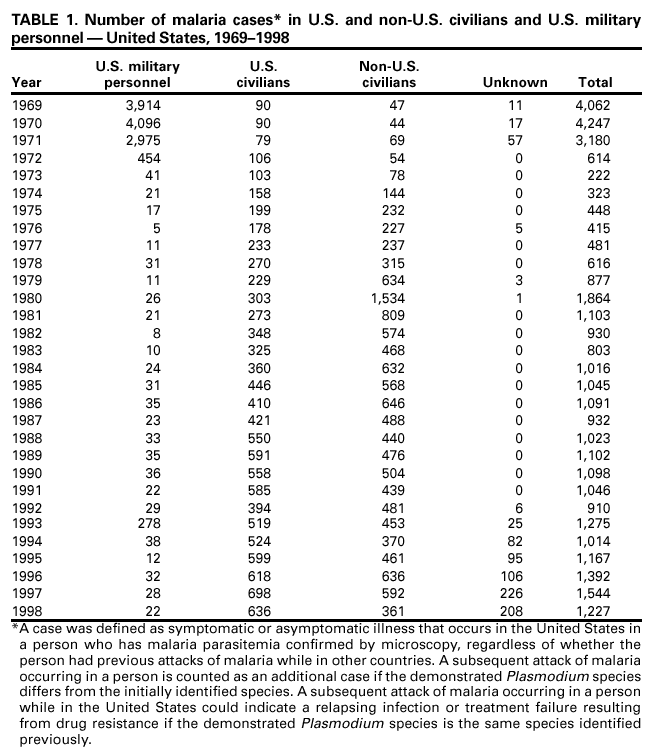
CDC received reports of 1,227 malaria cases with onset of symptoms in 1998,
among persons in the United States and its territories, representing a 20.5% decrease
from the 1,544 cases reported for 1997 (8). This incidence is the fourth highest
annual number of reported cases since 1980 and the second highest number of U.S.
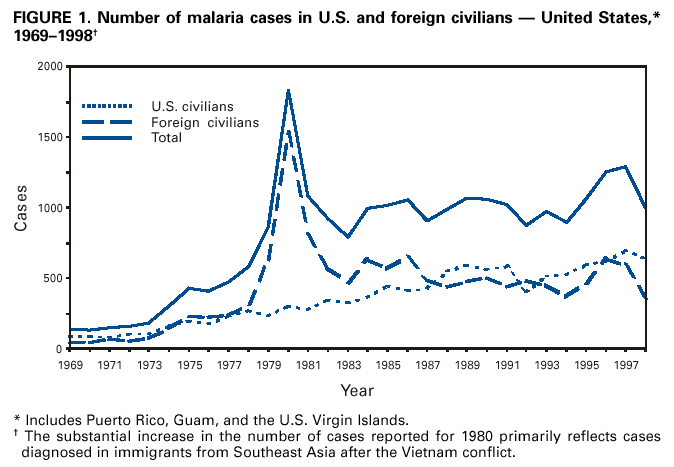
civilian cases reported in each year since 1968 (Table 1). In 1998, a total of 636
cases occurred among U.S. civilians, compared with 698 cases reported for 1997,
whereas the number of cases among non-U.S. civilians decreased from 592 cases to
361 (Figure 1). Cases among U.S. military personnel also decreased from 28 to 22
in 1998. In 208 cases, available information was insufficient to determine whether
the person was civilian or military personnel.
Plasmodium Species
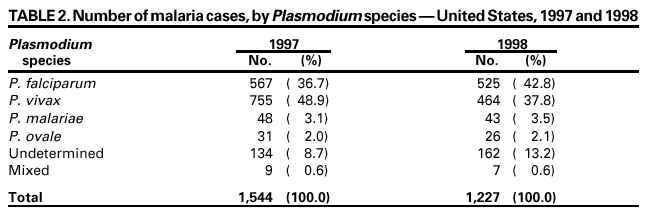
The infecting species of Plasmodium was identified in 1,065 (86.8%) cases reported
in 1998. P. falciparum and P. vivax were identified in blood smears from 42.8%
and 37.8% of infected persons, respectively (Table 2). The 464
P. vivax cases reported for 1998 represented a 38.5% decrease from the 755 cases reported in 1997. The
number of P.falciparum infections also decreased, but only by 7.4% (from 567 in 1997 to
525 in 1998). Among 1,202 cases in which both the region of acquisition and the
infecting species were known, 62.6% of infections acquired in Africa were attributed
to P. falciparum, and 14.2% were attributed to
P. vivax. For infections acquired in Asia and the Americas, 78.2% and 67.7%, respectively, were attributed to
P. vivax, and only 9.2% and 20.5% respectively, were attributed to
P. falciparum. A 56.7% decrease occurred (432 cases in 1997 to 187 cases in 1998) in
P. vivax cases acquired in Asia, a majority of which were acquired in India (371 cases in 1997 and 123 cases in 1998).
Imported Malaria Cases
Region of Acquisition and Diagnosis
Of all reported cases, 98% (n = 1,206) were classified as imported. Of 1,197
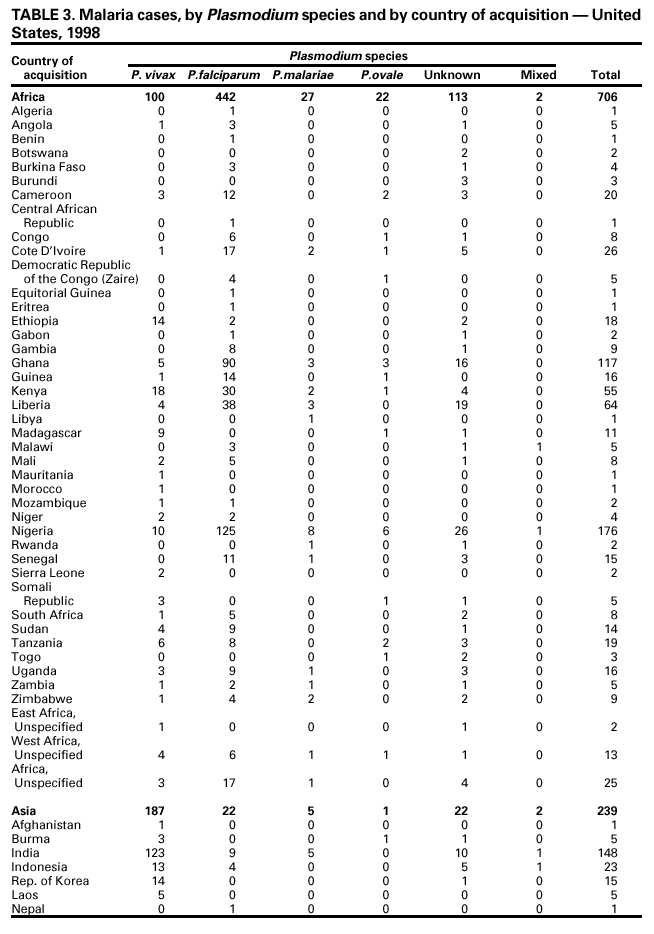
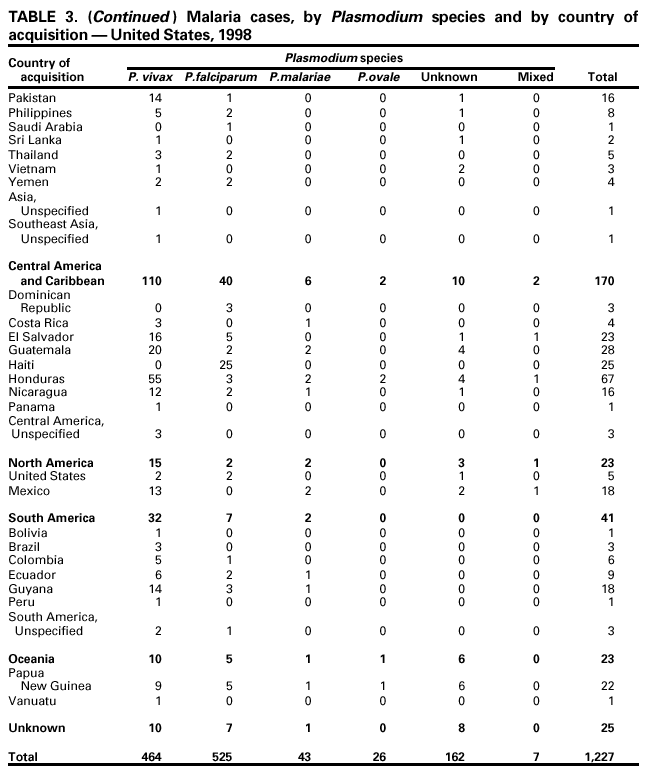
imported cases in which the region of acquisition was known, 60% (n = 706) were acquired
in Africa, 20% (n = 239) in Asia, and 19.1% (n = 229) in the Americas (Table 3).
The
highest proportion of cases acquired in Africa , 65.2% (n = 460), came from
countries in West Africa. The majority of cases acquired in Asia came from the
Indian subcontinent 61.9% (n = 148). The other regions where imported cases of
malaria were acquired were Central America and the Caribbean 14.2% (n = 170);
South America 3.4% (n = 41); Oceania 1.9% (n = 23); and Mexico 1.5% (n = 18).
Reported malaria cases acquired in Africa increased by 1.3% (n = 706) compared with
1997, and cases acquired in Asia decreased by 52.1% (n = 239) compared with 1997.
Cases from the Americas decreased by 6.5% (n =
229) compared with 1997.
In the United States, the seven areas reporting the highest number of malaria
cases were California (n = 232), New York City (n = 228), Minnesota (n = 83), New York
State (n = 75), Illinois (n = 62), Virginia (n = 54), and Florida (n = 47) (Figure 2).
When compared with 1997, each of these areas reported fewer cases in 1998, except
for Minnesota, which reported an increase to 83 from 60 cases in 1997. The
overall decrease in reported number of cases might be a result of decreased
international travel or immigration, improved use of chemoprophylaxis, or less
sensitive surveillance.
Interval Between Arrival and Onset of Symptoms
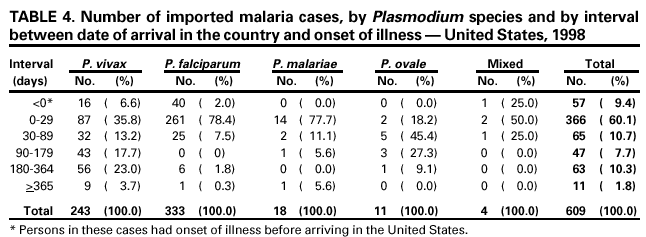
The interval between persons arriving in the United States and onset of symptoms
as well as the infecting Plasmodium species was known for 609 (50.5%) of the
imported cases of malaria (Table 4). Symptoms began after arrival in the United States for
552 (90.6%) of these persons. Clinical malaria developed in persons within 1 month
after their arrival in 261 (78.4%) of the 333 P.
falciparum cases and in 87 (35.8%) of the 243
P. vivax cases (Table 4). Only 11 (1.8%) persons reported the onset of symptoms
>1 year after returning to the United States. A total of 57 (9.4%) persons reported
the onset of symptoms before arriving in the United States.
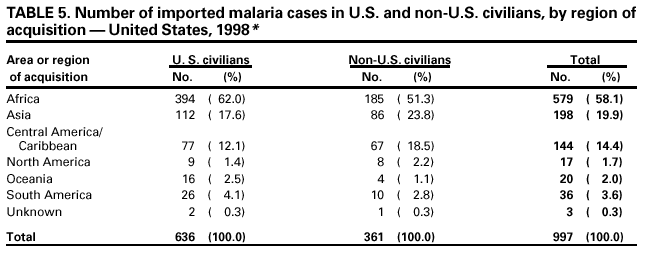
Imported Malaria Among U.S. and Non-U.S. Civilians
During 1998, a total of 997 imported malaria cases was reported among civilians.
Of these, 636 (63.8%) occurred among U.S. residents, and 361 (36.2%) occurred
among residents of other countries (Table 5). Of the 636 imported malaria cases among
U.S. civilians, 394 (62.0%) were acquired in Africa, an increase of 11.6% from the
cases reported in 1997. An additional 112 (17.6%) cases were acquired in Asia. The
Central American and Caribbean region was the reported source of 77 (12.1%) cases
of imported malaria among U.S. civilians.
Among 361 imported cases among non-U.S. civilians, 51.2% (n = 185) were
acquired in Africa; 23.8% (n = 86), Asia; and 18.6% (n = 67), Central America and
the Caribbean. The number of cases among non-U.S. civilians acquired in
Asia (particularly in India) decreased 70.8%, from 295 cases in 1997 to 86 cases in 1998.
Imported Malaria Among Military Personnel
A total of 22 cases of imported malaria among U.S. military personnel were
reported for 1998. This represents a 21% decrease from 28 cases reported among U.S.
military personnel in 1997.
Use of Antimalarial Chemoprophylaxis
Use of Chemoprophylaxis Among U.S. Civilians
Information concerning the use of chemoprophylaxis and area of travel was
known for 584 (91.8%) of the 636 U.S. civilians who had imported malaria. Of
these 584 persons, 347 (59.4%) had not taken any chemoprophylaxis, and 78 (13.4%)
had not taken the CDC-recommended drug for the area(s) visited. Only 126 (21.6%)
U.S. civilians had taken a medication recommended by CDC
(9). For the remaining 33
(5.6%) travelers, data regarding the drug taken were missing. A total of 104 of the
126 U.S. civilian patients who took CDC-recommended chemoprophylaxis had
taken mefloquine weekly; nine had taken doxycycline daily; and 13, who had traveled
only in areas where chloroquine-resistant malaria has not been documented, had
taken chloroquine weekly. Of the 78 patients taking a non-recommended drug,
information regarding the type of chemoprophylaxis used was known for 75. Of these 75
persons, 64 (85.3%) reported taking chloroquine and proguanil during travel to an area
where chloroquine resistance had been documented.
Use of Chemoprophylaxis Among Military Personnel
Of the 19 military personnel for whom information regarding chemoprophylaxis
use was available, 11 (57.9%) were not using any chemoprophylaxis. In 1997,
by comparison, 10 of 26 (38.4%) military case-patients for whom information
on chemoprophylaxis was available, had not used any chemoprophylaxis.
Malaria Infection After Using Recommended Chemoprophylaxis
A total of 155 (126 U.S. civilians, seven persons in the U.S. military, five
non-U.S. civilians, and 17 persons with missing information) acquired malaria after
taking recommended antimalarial chemoprophylaxis. The infecting species could not
be determined for 24 (15.5%) patients.
Of the 155 patients who acquired malaria after using
recommended chemoprophylaxis, 87 cases (53.5%) were caused by
P. vivax (n = 83) or P. ovale (n = 4). The remaining 44 cases of malaria reported among persons who had taken
a recommended antimalarial chemoprophylaxis included 39 cases of
P. falciparum, 4 of P. malariae, 1 of mixed infection
(P. falciparum and P. vivax), and 24 in which
the infecting species was not identified.
P. vivax or P. ovale Cases
Malaria case surveillance reports indicated that 15 (17.2%) of 87 patients with
P. vivax or P. ovale did not complete their antimalarial chemoprophylaxis as recommended.
A total of 54 (50.6%) cases of P. vivax or P.
ovale occurred >45 days after persons arrived in the United States. These cases were consistent with relapsing
infections and, thus, do not necessarily indicate chemoprophylaxis failures. Because
of insufficient information regarding 34 cases, no determination could be
made regarding whether these persons had relapsing infections. Nine cases of
P. vivax occurred <45 days after the person returned to the United States. Of these
persons, two did not complete their antimalarial chemoprophylaxis as recommended.
The region of acquisition varied for the seven persons who had
completed chemoprophylaxis as recommended (i.e., one from Central America, four from
South America, two from southeast Asia). No blood specimens were available to
check serum drug levels for any of these persons. These apparent
chemoprophylaxis failures might have been caused by inadequate dosing or unreported failure
to complete the recommended chemoprophylaxis regimen. These data are
insufficient to indicate new areas of chloroquine-resistant
P. vivax.
P. falciparum Cases
Among 39 cases of P. falciparum where persons reported taking
recommended antimalarial chemoprophylaxis, 36 acquired infection in Africa, one in Papua
New Guinea, and two in Central America and the Caribbean. Twelve (30.8%) of
these persons reported not completing their chemoprophylaxis as recommended. Two
of these 12 persons had high density parasitemia and required exchange
blood transfusion. A total of 27 (69.2%) persons acquired
P. falciparum infections despite
reportedly taking the recommended chemoprophylaxis regimen as
directed. However, serum drug levels were unavailable for these persons. These
failures might have been caused by inappropriate dosing or failure to complete
the recommended regimen.
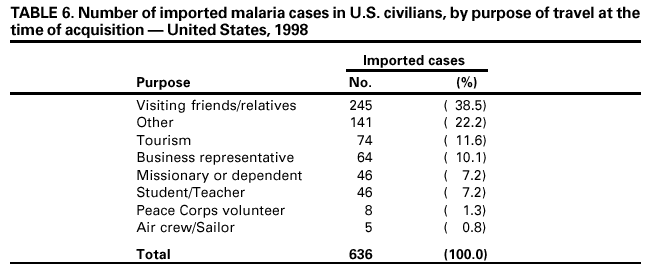
Purpose of Travel
The purpose of travel to malarious areas was reported for 495 (77.8%) of the
636 U.S. civilians with imported malaria (Table 6). Of cases among U.S. civilians,
the largest percentage (38.5%) occurred among persons who were visiting friends
or relatives in malarious areas; 11.6% and 10.1% of persons had traveled for
tourism and business purposes, respectively.
Malaria Acquired in the United States
Congenital Malaria
Case 1. On August 19, 1998, a full-term infant was born by spontaneous
vaginal delivery in Arizona. His parents were Ethiopian immigrants. During
September--November 1997, they had returned to Ethiopia. In January 1998,
P. vivax was diagnosed in the infant's mother and she was treated with chloroquine but was
not administered primaquine because she was pregnant. In May 1998, she
experienced a relapse of P. vivax and was retreated with chloroquine, and then
administered chloroquine weekly for chemoprophylaxis until delivery. The woman
discontinued chloroquine 4 weeks before delivery because of concerns regarding the
drug's potential adverse effects on the fetus. At the time of delivery, she experienced
high fevers and rigors. Repeat blood smears indicated
P. vivax, and after delivery she was treated with chloroquine and primaquine. A blood smear was not performed on
the newborn, and he was not treated at the time of delivery.
On September 7, the 18-day-old infant was hospitalized with a 1-day history of
fever and refusal to feed. His physical examination and laboratory tests were
normal. However, a blood smear revealed P.
vivax with 3% parasitemia and mature gametocytes. The infant was treated with chloroquine and the density of
his parasitemia decreased to 1% after 1 day. He improved clinically and was
discharged September 9.
Cryptic Malaria
Case 1. On July 17, 1998, a woman aged 63 years, from Virginia, reported
fever, myalgia, stiff neck, and diarrhea. Her family noted that she appeared less
coherent than usual. She experienced high fever and somnolence and was admitted to
the hospital on July 19. At the time of admission to a hospital, laboratory tests
were normal except for thrombocytopenia. On July 20,
P. falciparum was identified by a blood smear examination. She responded well to 7 days of quinine and
doxycycline. The patient was born in the United States and had no history of international
travel. She reported no history of previous malaria infection, transfusion of blood or
blood products, organ transplantation, or injection-drug use.
The state health department and CDC conducted epidemiologic and
environmental investigations to identify additional cases of locally acquired malaria. Active
case finding was conducted in surrounding counties, including a serologic study of
88 migrant farm workers living and working near the patient's residence. No
additional cases of malaria were reported. An environmental investigation using
larval collections, light traps, and landing collections
identified A. quadrimaculatus group, A. crucians sensu
strictu, and A. punctipennis (10). All are competent
malaria vectors. The source of infection was not determined.
Case 2. On October 3, 1998, a man aged 19 years was admitted to a hospital in
New Jersey after 10 days of nausea, vomiting, headaches, myalgia, cyclic fevers,
and jaundice. P. vivax parasites were identified on a routine complete blood count.
He was treated with chloroquine, and responded rapidly. Upon discharge, a
14-day course of primaquine was administered. The patient reported no history of
receiving a blood transfusion or blood products, organ transplantation, or injection-drug
use. His only international travel was a trip to the United Kingdom when he was aged
14 years. He lived with his parents and reported spending many summer nights in
the back yards of his house and the houses of friends in the neighborhood.
No epidemiologic or environmental investigation was performed.
Case 3. On December 15, 1998, a man aged 69 years was evaluated at a clinic
in Georgia with a 1-day history of fever. CDC confirmed the diagnosis of
P. vivax parasitemia in his blood smears. He responded well to treatment with
chloroquine and primaquine.
The patient had last traveled to a malarious area 10 years before the onset
of symptoms. He had no history of transfusion with blood or blood products,
organ tranplantation, or injection-drug use. However, he worked as an entomologist in
a laboratory where he routinely handled infecting anopheline mosquitoes. Before
his infection, he was working with anopheline mosquitoes infective with a strain of
P. vivax from southeast Asia and a West African strain of
P. ovale. In April 1996, the patient had experienced a similar episode of probable mosquitoborne
P. vivax malaria (11). In 1998, the infection was believed to have been acquired
through mosquitoborne transmission in the laboratory, but was classified as cryptic because
it could not be linked epidemiologically to other cases.
Induced Malaria
Case 1. On January 15, 1998, a man aged 49 years, who had a history
of hypertension, sickle cell disease, and a splenectomy, had hip replacement
revision surgery in Pennsylvania for avascular necrosis of the hip. He received four units
of packed red blood cells during surgery, but the procedure was otherwise
without complications. On February 1, he noted fever and chills. After several visits to
his orthopedic clinician and two emergency department visits, he was seen again
on February 19 in a hospital emergency department because of fever, hypotension,
and acute renal failure. P. falciparum with a parasitemia of 12% was identified on
blood smear. The patient was admitted to the intensive care unit (ICU) and treated
with parenteral quinidine, doxycycline, and 12 units of exchange blood
transfusion. Clinically, he responded well; his parasitemia decreased to 1% after 1 day of
therapy, and his renal function returned to baseline after 5 days. He was discharged after
7 days.
The patient had no history of international travel or injection-drug use. He
had received blood products from four separate donors in January 1998. Stored
serum samples from all donors were serologically tested by using indirect
fluorescent antibody test (IFA). Results from three donors were negative. One donor's (Donor
N) serum demonstrated elevated titers of antibodies to malaria
(P. falciparum, 1:16,384; P.
malariae 1:16,384; P. ovale 1:1,024;
and P. vivax 1:256). Polymerase chain
reaction performed on a sample of Donor N's blood, which was taken at the time of
donation, subsequently detected P.
falciparum DNA (12).
On the basis of the investigation, the patient likely acquired his
P. falciparum infection from the transfused unit of packed red blood cells donated by Donor N. Donor N
was
born in Nigeria, had lived in Europe, and had returned to Nigeria, where he lived
for approximately 20 years before immigrating to the United States in 1996. The
donor could not be located for treatment.
Deaths Attributed to Malaria
Case 1. On February 7, 1998, a man aged 42 years returned to North Carolina after
a 6-month photography assignment in Zimbabwe. He reported taking no
antimalarial chemoprophylaxis during his business trip. On February 11, the patient
began experiencing fever, chills, and myalgia that he ascribed to a viral syndrome
and influenza. He did not seek medical care during the subsequent 7 days, despite
a worsening of symptoms. On February 18, after reporting not feeling well, the
patient collapsed at home in his bathtub and was comatose when taken to a local
hospital emergency department. He was intubated, started on dopamine and
norepinephrine infusions, and underwent pericardiocentesis. He was airlifted to a nearby tertiary
care center where he died from cardiac arrest soon after arrival. Results from
testing performed at the emergency department
revealed P. falciparum ring forms on blood smears and evidence of intravascular hemolysis. An autopsy report listed his
cause of death as acute cerebral malaria caused by
P. falciparum. He also had evidence of cardiomegaly, pericardial effusion, renal failure, hepatomegaly, and splenomegaly.
Case 2. On July 5, 1998, a man aged 39 years returned to Hawaii from a 2-week
trip to the Philippines. He reported taking no antimalarial chemoprophylaxis during
his trip. Soon after arrival, he complained of fever and chills. A diagnosis of an
upper respiratory tract infection by a health-care provider was treated with an
unknown antibiotic and cough preparation. On July 7, he was brought to the hospital
with lethargy after a witnessed generalized
seizure at home. In the emergency department, he was unresponsive, jaundiced, and had dark-colored urine.
He experienced another witnessed seizure and required intubation for
respiratory support. Test results from a lumbar puncture and computed tomography (CT) scan
of the head were normal, as was his complete blood
count. P. falciparum ring forms were found on a blood smear. He was admitted to ICU and placed on
intravenous quinidine.
The patient remained in the intensive care unit for a prolonged period.
His parasitemia decreased after 7 days of quinidine therapy, but the patient continued
to need respiratory support. The patient also received primaquine therapy. His
mental status wavered, and at one point, he became alert for a short period. On July 16,
he developed Pseudomonas pneumonia and his mental status worsened.
Serial electroencephalograms (EEGs) revealed diffuse global slowing and suppression
of generalized frequencies. He also required four units of packed red blood cells
for severe anemia. The patient died on July 25 from pneumonia, renal failure,
hepatitis, and sequelae of cerebral malaria.
Case 3. On September 1, 1998, a male resident of Ghana, aged 61 years
with noninsulin-dependent diabetes mellitus and asthma, arrived in Michigan to
attend his daughter's wedding. He had been out of the United States for 2 years
and reported taking no malaria chemoprophylaxis. He reported taking
intermittent prednisone for asthma control. On September 2, he visited a clinic in a local
hospital to obtain a new glucometer and was noted to have severe rigors. He reported a
2-week history of weakness and chills that had been evaluated in Ghana and
diagnosed as a viral syndrome. He was evaluated in the hospital emergency department
and admitted for observation in an isolation room because he had a patchy right
upper
lobe infiltrate indicative of tuberculosis. He had no other symptoms, and
on admission his standard laboratory test values were normal.
On September 4, hospital staff members found the patient unresponsive
and incontinent in his room. He required intubation and was comatose when
transferred to the intensive care unit. Blood smears taken on admission were returned at
that time and revealed rare P. falciparum ring forms. Blood smears performed in
ICU indicated a parasitemia of 25%. Intravenous quinidine was initiated, and the
dose was adjusted for moderate renal failure. A head CT showed cerebral edema and
a loss of gray matter/white matter distinction. Although the patient's parasitemia
level decreased to 10% after 48 hours of parenteral quinidine therapy, his clinical
condition did not improve, and he never regained consciousness. He died September 10.
Case 4. On November 28, 1998, a woman aged 68 years with no detailed
previous medical history returned to New York City after spending 3 weeks in Liberia
visiting friends and relatives. She reported taking no antimalarial chemoprophylaxis.
Soon after her return, she began experiencing fevers, chills, and cough. On December
9, she sought medical attention and was prescribed amoxicillin. On December 11,
she was brought to the hospital for generalized weakness and hypotension.
Her diagnosis was pericarditis and IV antibiotics were administered.
P. falciparum ring forms were identified on a blood smear performed during admission, and she
was administered IV quinidine and doxycycline. She also was administered a
treatment dose of mefloquine. Her condition worsened rapidly, and she was intubated for
acute respiratory distress syndrome.
The patient remained in ICU for 4 weeks for respiratory support. On January 7,
1999, the patient underwent a tracheostomy procedure performed for
long-term ventilatory support. After the procedure, the patient experienced
cardiovascular complications and died.
DISCUSSION
In 1998, a total of 1,227 cases of malaria were reported to CDC, a decrease from
the 1,544 cases reported for 1997. This change resulted primarily from a decrease
in cases acquired in Asia that might have resulted from decreased
reporting, immigration, international travel, and transmission; and change in travel patterns,
or increased use of effective antimalarial chemoprophylaxis.
One reason for conducting malaria surveillance is to monitor the emergence of
drug resistance and the consequent failure of chemoprophylaxis. However,
approximately 73% of imported malaria cases among U.S. civilians occurred in persons who
were either not taking chemoprophylaxis or were taking chemoprophylaxis regimens
not recommended for the region they were traveling to or from. Of the 155 persons
who reported taking recommended chemoprophylaxis, 123 cases (i.e., 68
P. vivax, 27 P. falciparum, 19 unknown species, 4
P. ovale, 4 P. malariae, and 1 mixed
infection), insufficient information was available to determine whether cases
represented persons not completing antimalarial chemoprophylaxis as recommended,
errors made by health-care workers or laboratory staff members, or emerging
drug resistance. However, no conclusive evidence existed to indicate a single national
or regional source of infection among this group of patients.
The importance of taking proper precautions and chemoprophylaxis is indicated
by the four deaths attributed to malaria in the United States in 1998. None of
the patients had taken prophylaxis; two had substantial delays in seeking care; and
three were treated for a nonmalaria illness before it was determined they had malaria.
This
pattern is consistent with previous findings from a review of deaths attributed
to malaria in the United States (13).
Signs and symptoms of malaria can be vague, but fever is generally present.
Other symptoms include headache, chills, increased sweating, back pain, myalgia,
diarrhea, nausea, vomiting, and cough. Prompt diagnosis requires that malaria be included
in the differential diagnosis of infection in a febrile person with a recent history of
travel to a malarious area. Clinicians should ask febrile patients for a travel
history, particularly when evaluating febrile illnesses in international visitors,
immigrants, refugees, migrant laborers, and international travelers.
Treatment for malaria should be initiated immediately after the diagnosis has
been confirmed by a positive blood smear. Treatment should be determined on the
basis of the infecting Plasmodium species, the probable geographic origin of the
parasite, the parasite density, and the patient's clinical status
(14). Although non-falciparum malaria rarely causes complications,
P. falciparum malaria can cause severe, life-threatening complications.
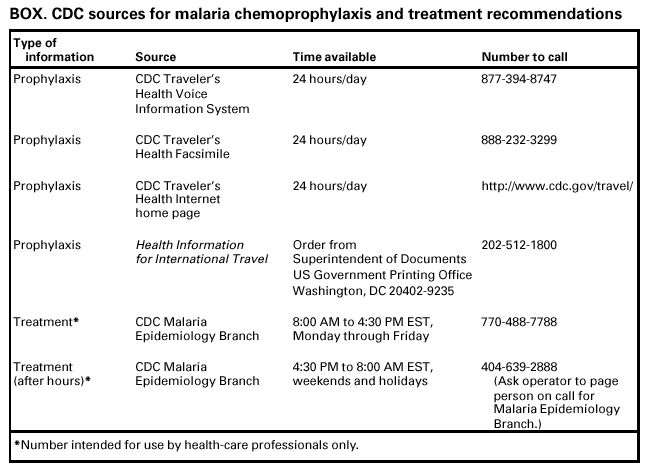
Healthcare workers are encouraged to consult appropriate sources for
malaria treatment recommendations and suspected chemoprophylaxis failure or call
CDC's National Center for Infectious Diseases, Division of Parasitic Diseases,
Malaria Epidemiology Branch. Detailed recommendations for preventing malaria
are available 24 hours a day by calling 877-FYI-TRIP or from the CDC Traveler's
Health website at <http://www.cdc.gov/travel>. In addition, CDC publishes annually
updated recommendations in Health Information for International
Travel (9) (Box).
Acknowledgment
The authors thank state health departments, health-care providers, and laboratories
for reporting this information to CDC.
References
World Health Organization. World malaria situation in 1994. Wkly Epidemiol
Rec 1997;72:269--76.
Pan American Health Organization. Report for registration of malaria eradication from
the United States of America. Washington, DC: Pan American Health Organization, 1969.
Zucker JR. Changing patterns of autochthonous malaria transmission in the United
States: A review of recent outbreaks. Emerg Infect Dis 1996; 2;1:37--43.
MacArthur JR, Holtz TH, Jenkins J, et al. Probable locally acquired
mosquito-transmitted malaria in Georgia, 1999. Clin Infect Dis 2001;32e:124--8.
Lackritz EM, Lobel HO, Howell J, Bloland P, Campbell CC. Imported
Plasmodium falciparum malaria in American travelers to Africa: implications for prevention
strategies. JAMA 1991; 265(3):383--5.
Stroup DF. Special analytic issues. In: principles and practice of public health
surveillance. Teutsch SM and Churchill RE, eds. New York, NY: Oxford University Press, 1994:143--5.
World Health Organization. Terminology of malaria and of malaria eradication.
Geneva, Switzerland: World Health Organization, 1963:32.
Centers for Disease Control and Prevention. Health information for international
travel, 1999--2000. Atlanta, Georgia: US Department of Health and Human Services, CDC, 1999.
Strickman D, Gaffigan TS, Wirtz RA, et al. Mosquito collections following
local transmission of Plasmodium falciparum malaria in Westmoreland County, Virginia. Journal
of the American Mosquito Control Association 2000; 16;3:219--22.
Greenberg AE, Lobel HO. Mortality from
Plasmodium falciparum malaria in travelers
from the United States, 1959--1987.Ann Intern Med 1990; 113;4:326--27.
Zucker JR, Campbell CC. Malaria: principles of prevention and treatment. Infect Dis
Clin NorthAm 1993; 7(3):547--67.
* To obtain confirmation diagnosis of blood smears from questionable cases and to
obtain appropriate treatment recommendations, contact either your state or local health
department or CDC's National Center for Infectious Diseases, Division of Parasitic Diseases,
Malaria Epidemiology Branch (Box).
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.