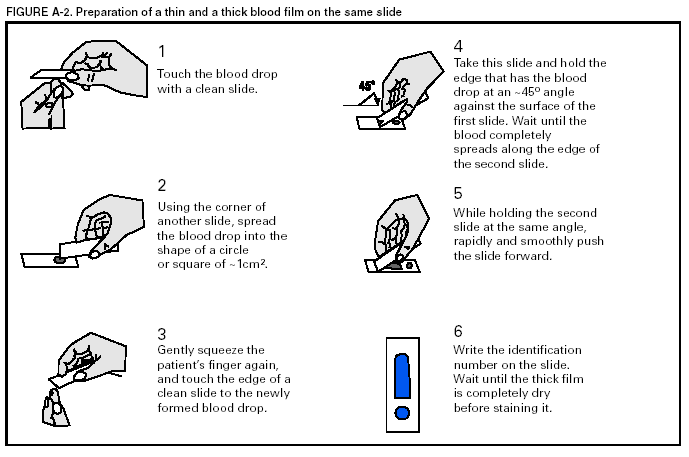
To establish the diagnosis of malaria, a blood film must be prepared from fresh blood obtained by pricking the
patient's finger (Figures A-1 and A-2).* The thin film is fixed in methanol before staining; the thick film is stained unfixed.
Certain
hospitals have a Wright-Giemsa stain available, which is acceptable; however, Wright stain alone will not reliably
indicate Plasmodium parasites. For best results, the film should be stained with a 3% Giemsa solution (pH of 7.2) for 30--45
minutes. In P. falciparum infections, the parasite density should be estimated by counting the percentage of red blood cells infected
--- not the number of parasites --- under an oil immersion lens on a thin film.
Thick blood films are more sensitive in detecting malaria parasites because the blood is concentrated, allowing a
greater volume of blood to be examined. However, thick films are more difficult to read, and thin films might be preferred
by laboratories that have limited experience.
Plasmodium parasites are always intracellular, and they demonstrate, if
stained correctly, blue cytoplasm with a red chromatin dot. Common errors in reading malaria films are caused by platelets overlying a red blood cell, concern regarding missing a positive slide, and misreading artifacts as parasites. Persons suspected of
having malaria, but whose blood films do not indicate the presence of parasites, should have blood films repeated approximately every 12--24 hours for 3 consecutive days. If films remain negative, then the diagnosis of malaria is unlikely.
For rapid diagnosis, the thick and thin films should be made on separate slides. The thin film should be air-dried, fixed with methyl alcohol, and immediately stained. If no parasites are visible on the thin film, the laboratorian should wait until the thick film is dry, then examine it for organisms that might not have been detected on the thin preparation.
* In Figures A-1 and A-2, the hands are illustrated ungloved to better indicate their placement during the procedures. However, wearing gloves while processing blood specimens is recommended to prevent transmission of bloodborne pathogens
(MMWR 1988;37:377--82, 387--8 and MMWR 1987;36[No.
S2]).
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.