|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
Assisted Reproductive Technology Surveillance --- United States, 2005Please note: Errata have been published for this article. To view the errata, please click here and here. Victoria Clay Wright, MPH
Corresponding author: Victoria Clay Wright, MPH, Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, 4770 Buford Hwy., N.E., MS K-34, Atlanta, GA 30341. Telephone: 404-639-6220; Fax: 404-639-8615; E-mail: vwright@cdc.gov.
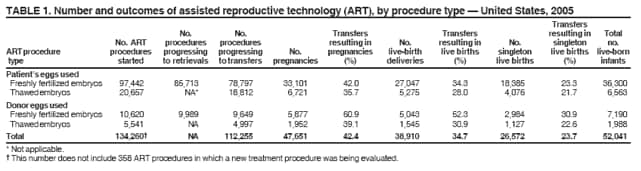
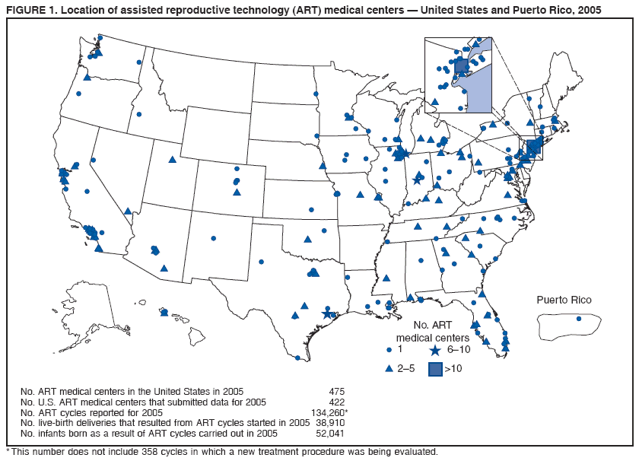
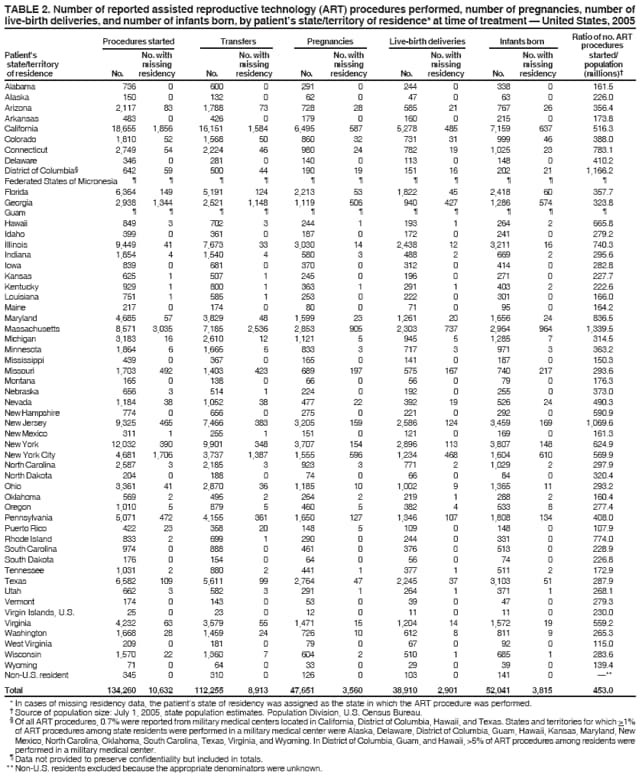
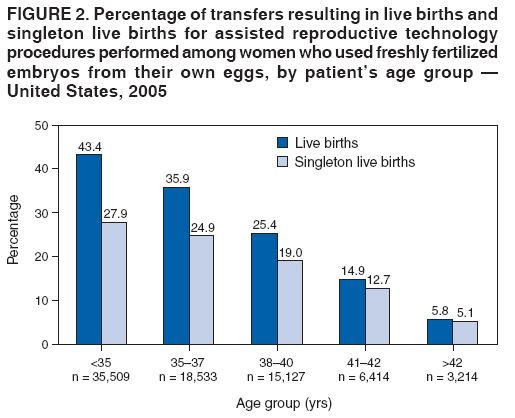
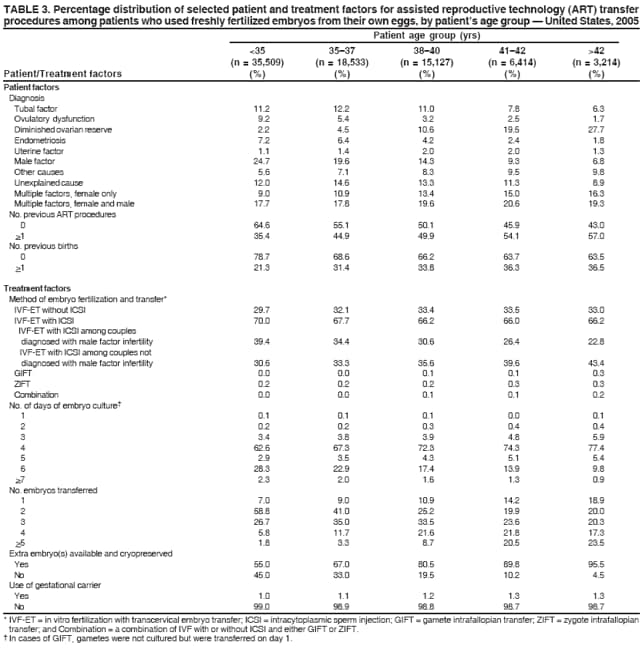
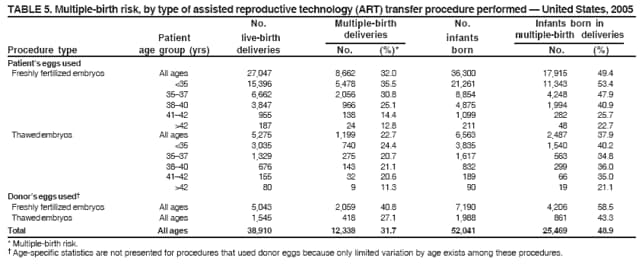
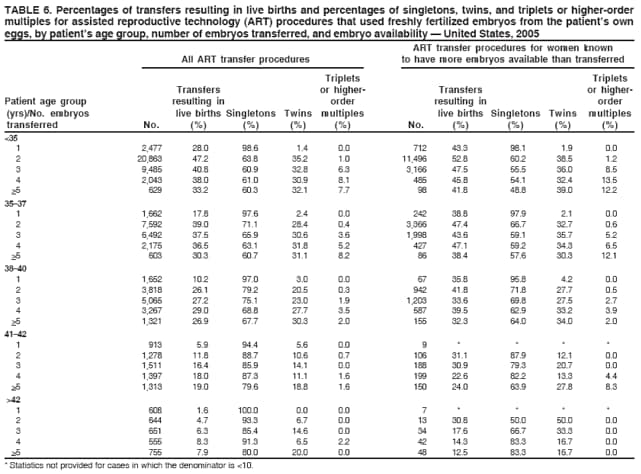
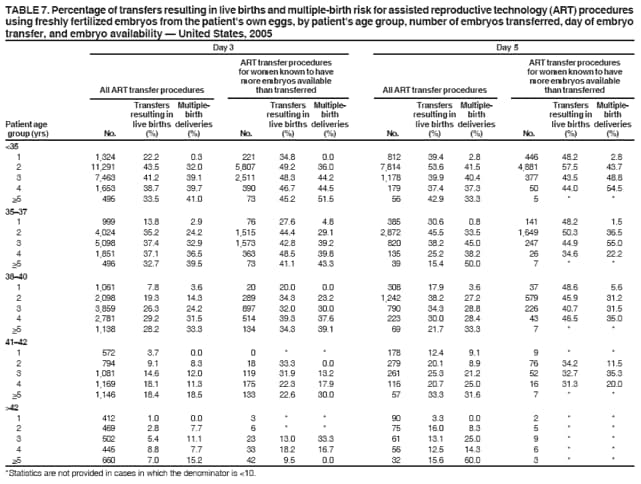
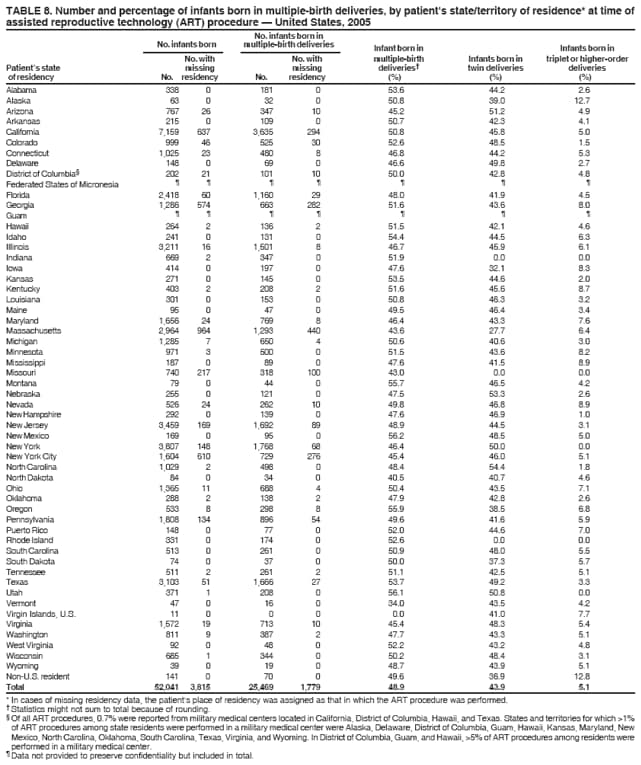
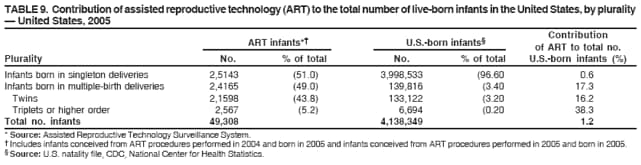
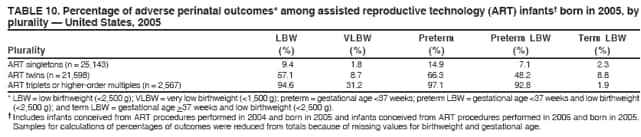
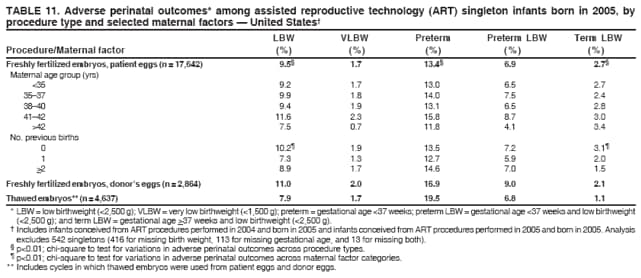
AbstractProblem/Condition: Assisted reproductive technology (ART) includes fertility treatments in which both eggs and sperm are handled in the laboratory (i.e., in vitro fertilization and related procedures). Patients who undergo ART procedures are more likely to deliver multiple-birth infants than women who conceive naturally. Multiple births are associated with increased risk for mothers and infants (e.g., pregnancy complications, premature delivery, low-birthweight infants, and long-term disability among infants). This report presents the most recent national data and state-specific results. Reporting Period Covered: 2005. Description of System: In 1996, CDC initiated data collection regarding ART procedures performed in the United States, as mandated by the Fertility Clinic Success Rate and Certification Act of 1992 (FCSRCA) (Public Law 102-493 [October 24, 1992]). Beginning with 2004, CDC has contracted with a statistical survey research organization, Westat, Inc., to obtain data from ART medical centers in the United States. Westat, Inc., maintains CDC's web-based data collection system called the National ART Surveillance System (NASS). Results: In 2005, a total of 134,260 ART procedures were reported to CDC. These procedures resulted in 38,910 live-birth deliveries and 52,041 infants. Nationwide, 73% of ART procedures used freshly fertilized embryos from the patient's eggs, 15% used thawed embryos from the patient's eggs, 8% used freshly fertilized embryos from donor eggs, and 4% used thawed embryos from donor eggs. Overall, 42% of ART transfer procedures resulted in a pregnancy, and 35% resulted in a live-birth delivery (delivery of one or more live-born infants). The highest live-birth rates were observed among ART procedures that used freshly fertilized embryos from donor eggs (52%). The highest numbers of ART procedures were performed among residents of California (18,655), New York (12,032), Illinois (9,449), New Jersey (9,325), and Massachusetts (8,571). These five states also reported the highest number of live-birth deliveries. Of 52,041 infants born through ART, 49% were born in multiple-birth deliveries. The multiple-birth risk was highest for women who underwent ART transfer procedures that used freshly fertilized embryos from either donor eggs (41%) or their own eggs (32%). Approximately 1% of U.S. infants born in 2005 were conceived through ART. Those infants accounted for 17% of multiple births nationwide. Approximately 9% of ART singletons, 57% of ART twins, and 95% of ART triplets or higher-order multiples were low birthweight. Similarly, 15% of ART singletons, 66% of ART twins, and 97% of ART triplets or higher-order multiples were born preterm. Interpretation: Whether an ART procedure resulted in a pregnancy and live-birth delivery varied according to different patient and treatment factors. ART poses a major risk for multiple births that are associated with adverse maternal and infant outcomes (e.g., preterm delivery, low birthweight, and infant mortality). This risk varied according to the patient's age, the type of ART procedure performed, the number of embryos available for transfer to the uterus, the number actually transferred, and the day of transfer (day 3 or day 5). Public Health Actions: ART-related multiple births represent a sizable proportion of all multiple births nationwide and in selected states. To minimize the adverse maternal and child health effects that are associated with multiple pregnancies, ongoing efforts to limit the number of embryos transferred in each ART procedure should be continued and strengthened. Adverse maternal and infant outcomes (e.g., low birthweight and preterm delivery) associated with ART treatment choices should be explained fully when counseling patients who are considering ART. IntroductionSince 1978, assisted reproductive technology (ART) procedures have been used to overcome infertility. ART procedures include those infertility treatments in which both eggs and sperm are handled in the laboratory for the purpose of establishing a pregnancy (i.e., in vitro fertilization [IVF] and related procedures). Since the birth of the first U.S. infant conceived with ART in 1981, use of these treatments has increased dramatically. Both the number of medical centers providing ART services and the number of procedures performed annually in the United States have steadily increased (1). In 1992, Congress passed the Fertility Clinic Success Rate and Certification Act (FCSRCA),* which requires each medical center in the United States that performs ART procedures to report data to CDC annually on every ART procedure initiated. CDC uses the data to report medical center--specific pregnancy success rates. In 1997, CDC published the first surveillance report under this mandate (2). That report was based on ART procedures performed in 1995. Since then, CDC has continued to publish a surveillance report annually that details each medical center's success rates. CDC also has used this surveillance data file to perform more in-depth analyses of infant outcomes (e.g., multiple births) (3--10). Multiple-infant births are associated with greater health problems for both mothers and infants, including higher rates of caesarean deliveries, prematurity, low birthweight, and infant death and disability (11,12). In the United States, ART has been associated with a substantial risk for multiple gestation pregnancy and multiple birth (3--10). In addition to the multiple-birth risks, studies suggest an increased risk for low birthweight among singleton infants conceived through ART (13,14). This report is based on ART surveillance data provided to CDC's National Center for Chronic Disease Prevention and Health Promotion, Division of Reproductive Health, regarding procedures performed in 2005. A report of these data, according to the medical center in which the procedure was performed, was published separately (1). In this report, emphasis is on presenting state-specific data and more detailed data regarding risks associated with ART (e.g., multiple birth, low birthweight, and preterm delivery). MethodsCDC contracted with Westat, Inc., to collect data on ART procedures performed in 2005 from medical centers in the United States and its territories. Data collected include patient demographics, medical history and infertility diagnoses, clinical information pertaining to the ART procedure, and information regarding resultant pregnancies and births. The data file is organized with one record per ART procedure performed. Multiple procedures from a single patient are not linked. Ninety percent of ART medical centers reported their 2005 data (1). The names of nonreporting programs were published as prescribed by the FCSRCA. ART data and outcomes from ART procedures are presented by patient's state of residence at time of treatment. If the patient's state of residency was missing, the state of residency was assigned as the state in which the ART procedure was performed. In addition, data regarding the number of ART procedures in relation to the total population for each state are indicated.† Data regarding number of procedures also are presented by treatment type and stage of treatment. ART procedures are classified into four groups according to whether the ART cycle involved the retrieval and fertilization of eggs (fresh cycle) or the thawing of previously frozen embryos (frozen cycle), and whether the eggs or embryos were those of the intended mother or were from a donor. Because both live-birth rates and multiple-birth risk vary substantially among these four treatment groups, data are presented separately for each type. In addition to treatment types, within a given treatment procedure, different stages of treatment exist. A typical ART procedure begins when a woman starts taking drugs to stimulate egg production or her ovaries are monitored with the intent of transferring embryos to her uterus. If eggs are produced, the procedure progresses to the egg retrieval stage. After the eggs are retrieved, they are combined with sperm in the laboratory (IVF), and if IVF is successful, the resulting embryos are selected for transfer. If the embryo implants in the uterus, a clinical pregnancy is diagnosed by the presence of a gestational sac detectable by ultrasound. Depending on the age of the mother, between 13% and 55% of clinical pregnancies are lost at a later point, mostly during the 12 weeks (16). Beyond 12 weeks of gestation, the pregnancy usually progresses to a live-birth delivery, which is defined as the delivery of one or more live-born infants. Only ART procedures involving freshly fertilized embryos include an egg-retrieval stage. ART procedures using thawed embryos do not include egg retrieval because eggs were fertilized during a previous procedure, and the resulting embryos were frozen until the current procedure. An ART procedure can be discontinued at any step for medical reasons or by the patient's choice. Although a typical ART procedure includes IVF of gametes, culture for >2 days, and embryo transfer into the uterus (i.e., transcervical embryo transfer), in certain cases, unfertilized gametes (eggs and sperm) or zygotes (early embryos [i.e., a cell that results from fertilization of the egg by a sperm]) are transferred into the fallopian tubes within 1--2 days of retrieval. These are known as gamete and zygote intrafallopian transfer (GIFT and ZIFT). Another variation is intracytoplasmic sperm injection (ICSI), in which IVF is accomplished by selection of a single sperm that is injected directly into the egg. This technique was developed originally for couples with male factor infertility but now is commonly used for an array of diagnostic groups. This report presents data for each of the four treatment types: freshly fertilized embryos from the patient's eggs, freshly fertilized embryos from donor eggs, thawed embryos from the patient's eggs, and thawed embryos from donor eggs. In addition, it provides detailed data for the most common treatment type, those using freshly fertilized embryos from the patient's eggs. These procedures account for >70% of the total number of ART procedures performed each year. For procedures that progressed to the embryo-transfer stage, the report presents the percentage distribution of selected patient and treatment factors and the success rates (defined as live-birth deliveries per ART-transfer procedure), according to the same patient and treatment characteristics. Patient factors included the age of the woman undergoing ART, whether she had previously given birth, the number of previous ART attempts, and the infertility diagnosis of both the female and male partners. The patient's age at the time of the ART procedure was grouped into five age groups: age <35 years, 35--37 years, 38--40 years, 41--42 years, and >42 years. Infertility diagnoses ranged from one factor in one partner to multiple factors in one or both partners, as follows:
|