|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
Recommendations for Identification and Public Health Management of Persons with Chronic Hepatitis B Virus InfectionPrepared by
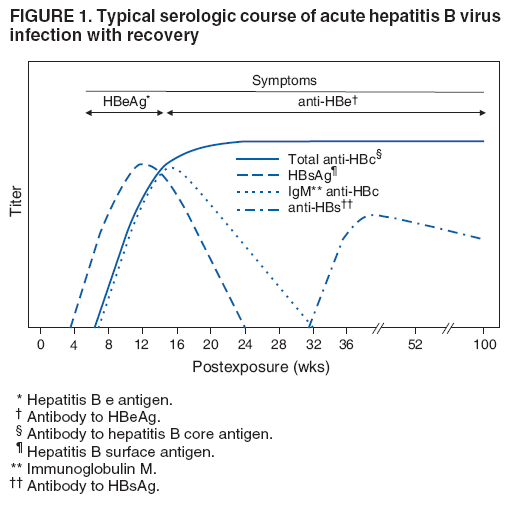
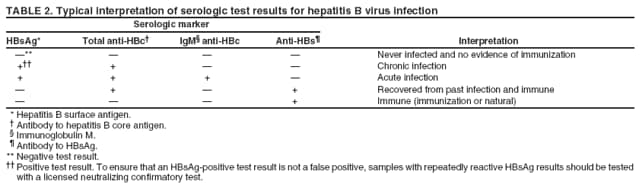
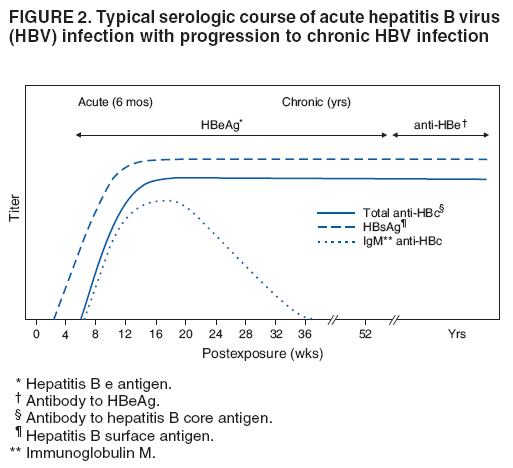
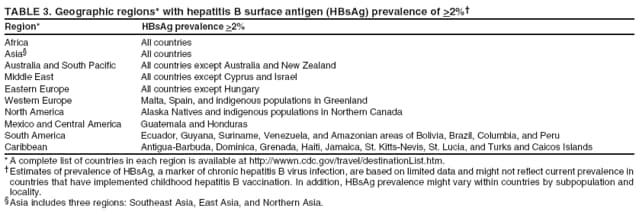
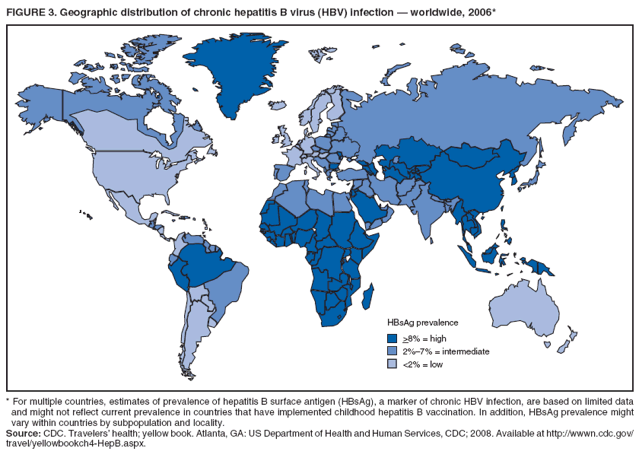
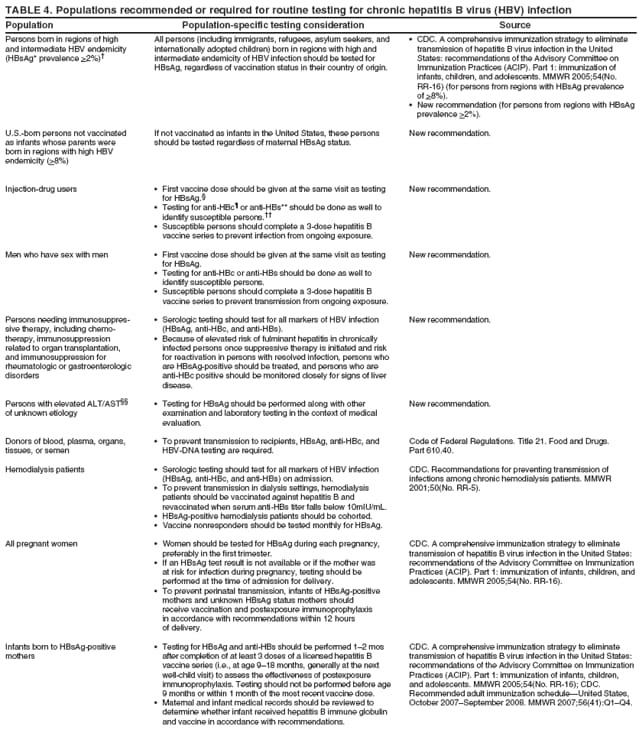
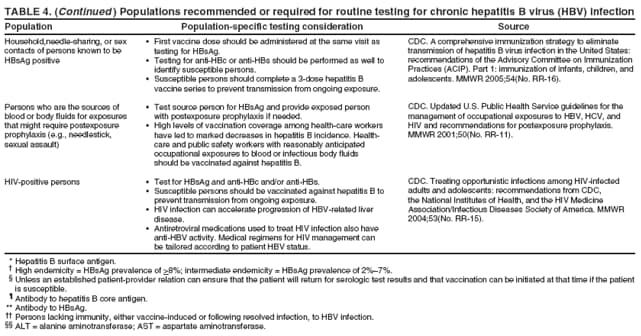
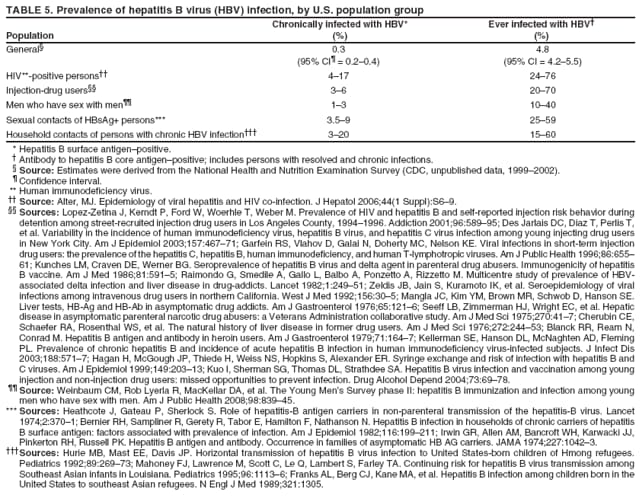
The material in this report originated in the National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Kevin Fenton, MD, Director, and the Division of Viral Hepatitis, John Ward, MD, Director. Corresponding preparer: Cindy M. Weinbaum, MD, Division of Viral Hepatitis, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, 1600 Clifton Road, MS G-37, Atlanta GA 30333. Telephone: 404-718-8596; Fax: 404-718-8595; email: chw4@cdc.gov. SummarySerologic testing for hepatitis B surface antigen (HBsAg) is the primary way to identify persons with chronic hepatitis B virus (HBV) infection. Testing has been recommended previously for pregnant women, infants born to HBsAg-positive mothers, household contacts and sex partners of HBV-infected persons, persons born in countries with HBsAg prevalence of >8%, persons who are the source of blood or body fluid exposures that might warrant postexposure prophylaxis (e.g., needlestick injury to a health-care worker or sexual assault), and persons infected with human immunodeficiency virus. This report updates and expands previous CDC guidelines for HBsAg testing and includes new recommendations for public health evaluation and management for chronically infected persons and their contacts. Routine testing for HBsAg now is recommended for additional populations with HBsAg prevalence of >2%: persons born in geographic regions with HBsAg prevalence of >2%, men who have sex with men, and injection-drug users. Implementation of these recommendations will require expertise and resources to integrate HBsAg screening in prevention and care settings serving populations recommended for HBsAg testing. This report is intended to serve as a resource for public health officials, organizations, and health-care professionals involved in the development, delivery, and evaluation of prevention and clinical services. IntroductionChronic infection with hepatitis B virus (HBV) is a common cause of death associated with liver failure, cirrhosis, and liver cancer. Worldwide, approximately 350 million persons have chronic HBV infection, and an estimated 620,000 persons die annually from HBV-related liver disease (1,2). Hepatitis B vaccination is highly effective in preventing infection with HBV and consequent acute and chronic liver disease. In the United States, the number of newly acquired HBV infections has declined substantially as the result of the implementation of a comprehensive national immunization program (3--5). However, the prevalence of chronic HBV infection remains high; in 2006, approximately 800,000--1.4 million U.S. residents were living with chronic HBV infection (Table 1), and hepatitis B is the underlying cause of an estimated 2,000--4,000 deaths each year in the United States (6). Improving the identification and public health management of persons with chronic HBV infection can help prevent serious sequelae of chronic liver disease and complement immunization strategies to eliminate HBV transmission in the United States. Persons with chronic HBV infection can remain asymptomatic for years, unaware of their infections and of their risks for transmitting the virus to others and for having serious liver disease later in life. Early identification of persons with chronic HBV infection permits the identification and vaccination of susceptible household contacts and sex partners, thereby interrupting ongoing transmission. All persons with chronic HBV infection need medical management to monitor the onset and progression of liver disease and liver cancer. Safe and effective antiviral agents now are available to treat chronic hepatitis B, providing a greater imperative to identify persons who might benefit from medical evaluation, management, and antiviral therapy and other treatment when indicated. The majority of the medications now in use for hepatitis B treatment were approved by the Food and Drug Administration (FDA) in 2002 or later; two forms of alfa 2 interferon and five oral nucleoside/nucleotide analogues have been approved, and other medications are in clinical trials. Serologic testing for hepatitis B surface antigen (HBsAg) is the primary way to identify persons with chronic HBV infection. Because of the availability of effective vaccine and postexposure prophylaxis, CDC previously recommended HBsAg testing for pregnant women, infants born to HBsAg-positive mothers, household contacts and sex partners of HBV-infected persons, persons born in countries with HBsAg prevalence of >8%, and persons who are the source of blood or body fluid exposures that might warrant postexposure prophylaxis (e.g., needlestick injury to a health-care worker or sexual assault), and persons infected with human immunodeficiency virus (HIV) (4,5,7--11). This report updates and expands these multiple previous CDC guidelines for HBsAg testing and includes new recommendations for public health evaluation and management of chronically infected persons and their contacts. Routine HBsAg testing now is recommended for persons born in geographic regions in which HBsAg prevalence is >2%, men who have sex with men (MSM), and injection-drug users (IDUs). MethodsDuring February 7--8, 2007, CDC convened a meeting of researchers, physicians, state and local public health professionals, and other persons in the public and private sectors with expertise in the prevention, care, and treatment of chronic hepatitis B. These consultants reviewed available published and unpublished epidemiologic and treatment data, considered whether to recommend testing specific new populations for HBV infection, and discussed how best to implement new and existing testing strategies. Topics discussed included 1) the changing epidemiology of chronic HBV infection, 2) health disparities caused by the disproportionate HBV-related morbidity and mortality among persons infected as infants and young children in countries with high levels of HBV endemicity, and 3) the increasing benefits of care and opportunities for prevention for infected persons and their contacts. On the basis of this discussion, CDC determined that reconsideration of current guidelines was warranted. This report summarizes current HBsAg testing recommendations published previously by CDC, expands CDC recommendations to increase the identification of chronically infected persons in the United States, and defines the components of programs needed to identify HBV-infected persons successfully. Clinical Features and Natural History of HBV InfectionHBV is a 42-nm DNA virus in the Hepadnaviridae family. After a susceptible person is exposed, the virus is transported by the bloodstream to the liver, which is the primary site of HBV replication. HBV infection can produce either asymptomatic or symptomatic infection. When clinical manifestations of acute disease occur, illness typically begins 2--3 months after HBV exposure (range: 6 weeks--6 months). Infants, children aged <5 years, and immunosuppressed adults with newly acquired HBV infection typically are asymptomatic; 30%--50% of other persons aged >5 years have clinical signs or symptoms of acute disease after infection. Symptoms of acute hepatitis B include fatigue, poor appetite, nausea, vomiting, abdominal pain, low-grade fever, jaundice, dark urine, and light stool color. Clinical signs include jaundice, liver tenderness, and possibly hepatomegaly or splenomegaly. Fatigue and loss of appetite typically precede jaundice by 1--2 weeks. Acute illness typically lasts 2--4 months. The case-fatality rate among persons with reported cases of acute hepatitis B is approximately 1%, with the highest rates occurring in adults aged >60 years (12). Primary HBV infection can be self-limited, with elimination of virus from blood and subsequent lasting immunity against reinfection, or it can progress to chronic infection with continuing viral replication in the liver and persistent viremia. Resolved primary infection is not a risk factor for subsequent occurrence of chronic liver disease or hepatocellular carcinoma (HCC). However, patients with resolved infection who become immunosuppressed (e.g., from chemotherapy or medication) might, albeit rarely, experience reactivation of hepatitis B with symptoms of acute illness (13--15). HBV DNA has been detected in the livers of persons without serologic markers of chronic infection after resolution of acute infection (13,16--19). The risk for progression to chronic infection is related inversely to age at the time of infection. HBV infection becomes chronic in >90% of infants, approximately 25%--50% of children aged 1--5 years, and <5% of older children and adults) (13,20--23). Immunosuppressed persons (e.g., hemodialysis patients and persons with HIV infection) are at increased risk for chronic infection (22). Once chronic HBV infection is established, 0.5% of infected persons spontaneously resolve infection annually (indicated by the loss of detectable HBsAg and serum HBV DNA and normalization of serum alanine aminotransferase [ALT] levels); resolution is rarer among children than among adults (13,24,25). Persons with chronic HBV infection can be asymptomatic and have no evidence of liver disease, or they can have a spectrum of disease, ranging from chronic hepatitis to cirrhosis or liver cancer. Chronic infection is responsible for the majority of cases of HBV-related morbidity and mortality; follow-up studies have demonstrated that approximately 25% of persons infected with HBV as infants or young children and 15% of those infected at older ages died of cirrhosis or liver cancer. The majority remained asymptomatic until onset of cirrhosis or end-stage liver disease (26). Persons with histologic evidence of chronic hepatitis B (e.g., hepatic inflammation and fibrosis) are at higher risk for HCC than HBV-infected persons without such evidence (27). Potential extrahepatic complications of chronic HBV infection include polyarteritis nodosa (28,29), membranous glomerulonephritis, and membranoproliferative glomerulonephritis (30). Serologic Markers of HBV InfectionThe serologic patterns of chronic HBV infection are varied and complex. Antigens and antibodies associated with HBV infection include HBsAg and antibody to HBsAg (anti-HBs), hepatitis B core antigen (HBcAg) and antibody to HBcAg (anti-HBc), and hepatitis B e antigen (HBeAg) and antibody to HBeAg (anti-HBe). Testing also can be performed to assess the presence and concentration of circulating HBV DNA. At least one serologic marker is present during each of the different phases of HBV infection (Figures 1 and 2) (31). Serologic assays are available commercially for all markers except HBcAg, because no free HBcAg circulates in blood. No rapid or oral fluid tests are licensed in the United States to test for any HBV markers. Three phases of chronic HBV infection have been recognized: the immune tolerant phase (HBeAg-positive, with high levels of HBV DNA but absence of liver disease), the immune active or chronic hepatitis phase (HBeAg-positive, HBeAg-negative, or anti-HBe-positive, with high levels of HBV DNA and active liver inflammation), and the inactive phase (anti-HBe positive, normal liver aminotransferase levels, and low or absent levels of HBV DNA) (32). Patients can evolve through these phases or revert from inactive hepatitis B back to immune active infection at any time. The serologic markers typically used to differentiate among acute, resolving, and chronic infection are HBsAg, IgM anti-HBc, and anti-HBs (Table 2). The presence of HBeAg and HBV DNA generally indicates high levels of viral replication; the presence of anti-HBe usually indicates decreased or undetectable HBV DNA and lower levels of viral replication. In newly infected persons, HBsAg is the only serologic marker detected during the first 3--5 weeks after infection. The average time from exposure to detection of HBsAg is 30 days (range: 6--60 days) (31,33). Highly sensitive single-sample nucleic acid tests can detect HBV DNA in the serum of an infected person 10--20 days before detection of HBsAg (34). Transient HBsAg positivity has been reported for up to 18 days after hepatitis B vaccination and is clinically insignificant (35,36). Anti-HBc appears at the onset of symptoms or liver-test abnormalities in acute HBV infection and persists for life in the majority of persons. Acute or recently acquired infection can be distinguished from chronic infection by the presence of the immunoglobulin M (IgM) class of anti-HBc, which is detected at the onset of acute hepatitis B and persists for up to 6 months if the infection resolves. In patients with chronic HBV infection, IgM anti-HBc can persist during viral replication at low levels that typically are not detectable by the assays used in the United States. However, persons with exacerbations of chronic infection can test positive for IgM anti-HBc (37). Because the positive predictive value of this test is low in asymptomatic persons, IgM anti-HBc testing for diagnosis of acute hepatitis B should be limited to persons with clinical evidence of acute hepatitis or an epidemiologic link to a person with HBV infection. In persons who recover from HBV infection, HBsAg and HBV DNA usually are eliminated from the blood, and anti-HBs appears. In persons who become chronically infected, HBsAg and HBV DNA persist. In persons in whom chronic infection resolves, HBsAg becomes undetectable; anti-HBc persists and anti-HBs will occur in the majority of these persons (38,39). In certain persons, total anti-HBc is the only detectable HBV serologic marker. Isolated anti-HBc positivity can represent 1) resolved HBV infection in persons who have recovered but whose anti-HBs levels have waned, most commonly in high-prevalence populations; 2) chronic infection in which circulating HBsAg is not detectable by commercial serology, most commonly in high-prevalence populations and among persons with HIV or HCV infection (40) (HBV DNA has been isolated from the blood in <5% of persons with isolated anti-HBc) (40,41); or 3) false-positive reaction. In low-prevalence populations, isolated anti-HBc may be found in 10%--20% of persons with serologic markers of HBV infection, most of whom will demonstrate a primary response after hepatitis B vaccination(42,43). Persons positive only for anti-HBc are unlikely to be infectious except under unusual circumstances in which they are the source for direct percutaneous exposure of susceptible recipients to substantial quantities of virus (e.g., blood transfusion or organ transplant) (44). HBeAg can be detected in the serum of persons with acute or chronic HBV infection. In the majority of those with chronic infection, HBeAg is cleared over time, and anti-HBe appears (45--49). Presence of HBeAg correlates with more active disease: patients with HBeAg typically have high levels of HBV DNA (106--1010 IU/mL), whereas those who are HBeAg-negative and anti-HBe-positive generally have low or only modest HBV DNA levels (0--105 IU/mL). Epidemiology of HBV Infection in the United StatesTransmissionHBV is transmitted by percutaneous and mucosal exposure to infectious blood or body fluids. The highest concentrations of virus are found in blood; however, semen and saliva also have been demonstrated to be infectious (50). HBV remains viable and infectious in the environment for at least 7 days and can be present in high concentrations on inanimate objects, even in the absence of visible blood (13,51). Persons with chronic HBV infection are the major source of new infections, and the primary routes of HBV transmission are sexual contact, percutaneous exposure to infectious body fluids (such as occurs through needle sharing by IDUs or needlestick injuries in health-care settings), perinatal exposure to an infected mother, and prolonged, close personal contact with an infected person (e.g., via contact with exudates from dermatologic lesions, contact with contaminated surfaces, or sharing toothbrushes or razors), as occurs in household contact (5,52). No evidence exists of transmission of HBV by casual contact in the workplace, and transmission occurs rarely in childcare settings (4). Few cases have been reported in which health-care workers have transmitted infection to patients, particularly since implementation of standard universal infection control precautions (53). Incidence of HBV InfectionDuring 1985--2006, incidence of acute hepatitis B in the United States declined substantially, from 11.5 cases per 100,000 population in 1985 to 1.6 in 2006 (12). The actual incidence of new HBV infections is estimated to be approximately tenfold higher than the reported incidence of acute hepatitis B, after adjustment for underreporting of cases and asymptomatic infections. In 2006, an estimated 46,000 persons were newly infected with HBV (54). The greatest declines in incidence of acute disease have occurred in the cohorts of children for whom infant and adolescent catch-up vaccination was recommended (12). Among children aged <15 years, incidence of hepatitis B declined 98% during 1990--2006, from 1.2 per 100,000 population in 1990 to 0.02 in 2006 (12). This decline reflects the effective implementation of hepatitis B vaccination in the United States. Since 2001, fewer than 30 cases of acute hepatitis B have been reported annually in children born in 1991 or later, the majority of whom were international adoptees or children born outside the United States who were not fully vaccinated (55). In 2006, adults aged >20 years had the highest incidence of acute HBV infection, reflecting low hepatitis B vaccination coverage among adults with behavioral risks for HBV infection (e.g., MSM, IDUs, persons with multiple sex partners, and persons whose sex partners are infected with HBV) (12). Prevalence of HBV Infection and Its SequelaeU.S. mortality data for 2000--2003 indicated that HBV infection was the underlying cause of an estimated 2,000--4,000 deaths annually. The majority of these deaths resulted from cirrhosis and liver cancer (6; CDC, unpublished data, 2000--2003). The burden of chronic HBV infection in the United States is greater among certain populations as a result of earlier age at infection, immune suppression, or higher levels of circulating infection. These include persons born in geographic regions with high (>8%) or intermediate (2%--7%) prevalence of chronic HBV infection, HIV-positive persons (who might have additional risk factors) (56--58), and certain adult populations for whom hepatitis B vaccination has been recommended because of behavioral risks (e.g., MSM and IDUs). An accurate estimate of the prevalence of chronic HBV infection in the United States must be derived from multiple sources of data to account for the disproportionate contributions of persons of foreign birth, members of certain ethnic minority populations, and persons with certain medical conditions (Table 1). For the U.S.-born civilian noninstitutionalized population, prevalence estimates can be obtained from the most recent National Health and Nutrition Examination Survey (NHANES), which was conducted during 1999--2004 (available at http://www.cdc.gov/nchs/nhanes.htm). Because data from studies of foreign-born U.S. residents indicate that HBsAg seroprevalence corresponds to HBV endemicity in the country of origin (5), for the foreign-born population residing in the United States, HBV prevalence estimates were derived by applying country-specific prevalence estimates gathered from the scientific literature and the World Health Organization (2) to the number of foreign-born U.S. residents by their country of birth as reported by the 2006 U.S. Census American Community Survey (59). Other populations for which estimates were calculated included those in correctional institutions and the homeless. Together, these sources indicated that an estimated 800,000--1.4 million persons in the United States have chronic HBV infection. Approximately 0.3%--0.5% of U.S. residents are chronically infected with HBV; 47%--70% of these persons were born in other countries (Table 1). Global Variation in Prevalence of HBV Infection HBV transmission patterns and the seroprevalence of chronic HBV infection vary markedly worldwide, although seroprevalence studies in many countries are limited, and the epidemiology of hepatitis B is changing. Approximately 45% of persons worldwide live in regions in which HBV is highly endemic (i.e., where prevalence of chronic HBV infection is >8% among adults and that of resolved or chronic infection [i.e., anti-HBc positivity] is >60%) (2) (Figure 3). Historically, >90% of new infections occurred among infants and young children as the result of perinatal or household transmission during early childhood (26). Infant immunization programs in many countries have led to marked decreases in incidence and prevalence among younger, vaccinated members of these populations (60--63). Countries of intermediate HBV endemicity (i.e., HBsAg prevalence of 2%--7%) account for approximately 43% of the world's population; in these countries, multiple modes of transmission (i.e., perinatal, household, sexual, injection-drug use, and health-care--related) contribute to the infection burden. Regions of the world with high or intermediate prevalence of HBsAg include much of Eastern Europe, Asia, Africa, the Middle East, and the Pacific Islands (2,4) (Figure 3 and Table 3). In countries of low endemicity (i.e., HBsAg prevalence of <2%), the majority of new infections occur among adolescents and adults and are attributable to sexual and injection-drug--use exposures. However, in certain areas of low HBV endemicity, prevalence of chronic HBV infection is high among indigenous populations born before routine infant immunization (Table 3). In the United States, marked decreases in the prevalence of chronic HBV infection among younger, vaccinated foreign-born U.S. residents have been observed, most likely as a result of infant immunization programs globally (64). However, the rate of liver cancer deaths in the United States continues to be high among certain foreign-born U.S. populations. For example, the rate of liver cancer deaths is highest among Asians/Pacific Islanders, reflecting the high prevalence of chronic hepatitis B in this population (65,66). Globally, other regions with HBsAg prevalence of >2% also have identified high levels of HBV-associated HCC (67,68). Household Contacts and Sex Partners of Persons With Chronic HBV Infection Serologic testing and hepatitis B vaccination has been recommended since 1982 (69) for household contacts and sex partners of persons with chronic HBV infection because previous studies have determined that 14%--60% of persons living in households with persons with chronic HBV infection have serologic evidence indicating resolved HBV infection, and 3%--20% have evidence indicating chronic infection. The risk for infection is highest among unvaccinated children living with a person with chronic HBV infection in a household or in an extended family setting and among sex partners of chronically infected persons (70--77). Men Who Have Sex With Men During 1994--2000, studies of MSM aged <30 years identified chronic infection in 1.1% of MSM aged 18--24 years (95% confidence interval [CI] = 0--2.2%) (78), 2.1% (95% CI = 1.6%--2.6%) of MSM aged 15--21 years (79), and 2.3% (95% CI = 1.7%--2.8%) of MSM aged 22--29 years (80). In these studies, prevalence was higher (7.4%; 95% CI = 5.3%--9.6%) among young MSM who were HIV-positive than it was among those who were HIV-negative (1.5%; 95% CI = 1.2%--1.9%) (CDC, unpublished data, 2007). Before the introduction of the hepatitis B vaccine in 1982, prevalence of chronic HBV infection among MSM was 4.6%--6.1% (81--83). In recent studies, prevalence of past infection increased with increasing age, suggesting that chronic infection might still be more prevalent among older MSM (79,80). Injection-Drug Users Chronic HBV infection has been identified in 2.7%--11.0% of IDUs in a variety of settings (84--91); HBsAg prevalence of 7.1% (95% CI = 6.3%--7.8%) has been described among IDUs with HIV coinfection (92). IDUs contribute disproportionately to the burden of infection in the United States: in chronic HBV infection registries, 4%--12% of reported chronically infected persons had a history of injection-drug use (93). Prevalence of resolved or chronic HBV infection among IDUs increases with the number of years of drug use and is associated with frequency of injection and with sharing of drug-preparation equipment (e.g., cottons, cookers, and rinse water), independent of syringe sharing (94,95). HIV-Positive Persons As life expectancies for HIV-infected persons have increased with use of highly active antiretroviral therapy, liver disease, much of it related to HBV and HCV infections, has become the most common non-AIDS--related cause of death among this population (56,57,96,97). Chronic HBV infection has been identified in 6%--15% of HIV-positive persons from Western Europe and the United States, including 9%--17% of MSM; 7%--10% of IDUs; 4%--6% of heterosexuals; and 1.5% of pregnant women (58,98,99). This high level of chronic infection reflects both common routes of transmission for HIV and HBV and a higher risk of chronicity after HBV infection in an immunocompromised host (100--102). Persons With Selected Medical Conditions Although population-level studies are lacking to determine HBsAg prevalence among populations with other medical conditions, persons with chronic HBV infection who initiate cytotoxic or immunosuppressive therapy (e.g., chemotherapy for malignant diseases, immunosuppression related to organ transplantation, and immunosuppression for rheumatologic and gastroenterologic disorders) are at risk for HBV reactivation and associated morbidity and mortality (32,101,102). Prophylactic antiviral therapy can prevent reactivation and possible fulminant hepatitis in HBsAg positive patients (13,101). Rationale for Testing to Identify Persons With Chronic HBV InfectionAlthough limited data are available regarding the number of persons with chronic HBV infection in the United States who are unaware of their infection status, studies of programs conducting HBsAg testing among Asian-born persons living in the United States indicated that approximately one third of infected persons were unaware of their HBV infection (5,103--105). Published studies for other populations are lacking. Prompt identification of chronic infection with HBV is essential to ensure that infected persons receive necessary care to prevent or delay onset of liver disease and services to prevent transmission to others. Treatment guidelines for chronic hepatitis B have been issued (13,106,107), and multiple medications have been approved for treatment of adults with chronic HBV infection. With recent advances in hepatitis B treatment and detection of liver cancer, identification of an HBV-infected person permits the implementation of important interventions to reduce morbidity and mortality, including
|
![TABLE 1. Estimated number and percentage of hepatitis B surface antigen (HBsAg)�positive persons, by population segment �
United States, 2006
2006 HBsAg�positive persons
population HBsAg prevalence No.
Population segment (millions) (%) (thousands) (%)
U.S.-born, noninstitutionalized* 254.3 0.1 356 (30�50)
(95% CI� = 0.1�0.2) (229�534)
Foreign-born� 37.5 1.0�2.6 375�975 (47�70)
Correctional institutions� 2.2 2.0 44 (3�5)
Other group living quarters** 6 0.5 30 (2�3)
Total 300 0.3�0.5 805�1,405
* Source: 2006 American Community Survey, U.S. Census Bureau. Excludes persons living in correctional institutions and other group quarters. HBsAg
prevalence estimates were derived from the National Health and Nutrition Examination Survey (CDC, unpublished data, 2008).
� Confidence interval.
� Sources: 2006 American Community Survey, U.S. Census Bureau. Prevalence range represents estimates from the National Health and Nutrition
Examination Survey (1%) (CDC, unpublished data, 2008) and country-specific HBsAg estimates reported in the medical literature (2.6%) (CDC, unpublished
data, 2008), applied to the estimated population by country of origin. Infant immunization programs in many countries have led to marked
decreases in incidence and prevalence among younger, vaccinated members of these populations, which are largely not reflected in the medical
literature (Wasley A, Kruszon-Moran D, Kuhnert W, et al. Hepatitis B prevalence in the U.S. in era of vaccination [Abstract 723]. 45th Annual Meeting of
the Infectious Diseases Society of America, San Diego, California; October 4�7, 2007).
� Sources: Sabol WJ, Minton TD, Harrison PM. Prison and jail inmates at midyear 2006. Washington, DC: U.S. Department of Justice, Bureau of Justice
Statistics, Office of Justice Programs; 2007. Available at http://www.ojp.usdoj.gov/bjs/pub/pdf/pjim06.pdf. CDC. Prevention and control of infections
with hepatitis viruses in correctional settings. MMWR 2003;52(No. RR-1).
** Includes college dormitories, military quarters, nursing homes, group homes, and long-term care hospitals, as well as homeless persons. For persons
in other group-living quarters, estimated HBsAg prevalence was assumed to be equal to the mean prevalence in other groups. Source: 2006 American
Community Survey, U.S. Census Bureau.](figures/r708a1t1.gif)